Impact Factor ISSN: 1449-1907
- Issue 9; 2026
- Issue 8; 2026
- Issue 7; 2026
- Issue 6; 2026
- Issue 5; 2026
- Volume 23; 2026
- Past Issues
- Editorial Board
- Cover Images
- Index & Coverage
- Cover Suggestion
- Special Issues
Introduction
Methods
Results
Discussion
Supplementary Material
Declaration of Generative AI and...
Data Availability
References

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2026; 23(8):2540-2547. doi:10.7150/ijms.131856 This issue Cite
Research Paper
Interplay of Atrial Arrhythmia and Chronic Heart Failure: A Population-Based Analysis of Hospital Outcomes in Germany
Anastasia Janina Hobbach, MD1 ![]() , Jannik Feld, PhD2, Jürgen Reinhard Sindermann, MD1, Wolfgang Albrecht Linke, PhD3, Holger Reinecke, MD1
, Jannik Feld, PhD2, Jürgen Reinhard Sindermann, MD1, Wolfgang Albrecht Linke, PhD3, Holger Reinecke, MD1
1. Department of Cardiology I, Coronary, Peripheral Vascular Disease and Heart Failure, University Hospital Münster, Münster, Germany.
2. Institute of Biostatistics and Clinical Research, University of Münster, Münster, Germany.
3. Institute of Physiology II, University of Münster, 48149, Münster, Germany.
Received 2026-1-21; Accepted 2026-5-19; Published 2026-6-25
Abstract

Aims: Atrial fibrillation or flutter (AFl) frequently coexists with chronic heart failure (CHF), yet its impact on in-hospital outcomes in large, unselected populations remains insufficiently defined.
Methods: We analyzed all hospitalizations for CHF (ICD-10-GM I50*) in Germany from 2014 to 2022 using nationwide administrative data. Patients were stratified by rhythm status (AFl vs. non-AFl). Outcomes included in-hospital mortality, complications, length of stay, and health care costs. Multivariable logistic regression was used to identify independent predictors of mortality.
Results: Among 4,057,291 hospitalizations, 56.9% had AFl. These patients were older (median 82 vs. 79 years), more often female, and showed a higher comorbidity burden, particularly CKD, hypertension, and stroke. AFl was associated with higher rates of complications such as AKI (11.9% vs. 9.7%; p < 0.001) and cardiogenic shock (1.15% vs. 1.03%; p < 0.001), but lower use of mechanical ventilation and assist devices. Despite this, in-hospital mortality was slightly lower in AFl (8.30% vs. 8.66%). AFl patients had longer median hospital stays (8 vs. 7 days), while costs were comparable. Ventilated AFl patients had longer ventilation times (28 vs. 21 hours). In multivariable analysis, AFl was independently associated with higher mortality in most age groups, except for patients aged 40-49, 80-89, and > 90 years.
Conclusions: In this nationwide cohort, AFl was common among CHF patients and linked to more advanced disease. Its impact on in-hospital mortality was age-dependent and complex, highlighting the need for tailored clinical management.
Keywords: chronic heart failure, atrial fibrillation/flutter, in-hospital mortality, Germany, rhythm status, population-based cohort
Introduction
Chronic heart failure (CHF) and atrial fibrillation/flutter (AFl) are among the most prevalent and clinically significant cardiovascular diseases worldwide [1-2]. Their growing incidence and prevalence reflect not only an ageing population but also the persistence of shared risk factors such as arterial hypertension (AHT), diabetes mellitus (DM), and structural heart disease. Beyond their individual burden, both conditions are driving forces of health care utilization, characterized by frequent hospitalizations, recurrent outpatient consultations, and substantial socioeconomic costs [1,3].
The clinical impact of CHF and AFl extends beyond symptom burden and health care use. Each condition is independently associated with adverse prognosis, and their coexistence - found in up to 50% of heart failure (HF) patients [4] - is increasingly recognized as a distinct clinical entity with complex management challenges [5]. A bidirectional relationship has been established: AFl can lead to CHF through mechanisms such as tachycardia-induced cardiomyopathy, while structural and functional cardiac remodeling in CHF increases susceptibility to atrial arrhythmias [6]. Notably, this interplay is not confined to one specific CHF phenotype but affects patients across the spectrum of left ventricular (LV) ejection fraction (EF) [7].
Although prior studies have demonstrated that both optimal guideline-directed HF therapy and rhythm control strategies for AFl can improve clinical outcomes [6], the precise effect of atrial arrhythmia on in-hospital outcomes in patients hospitalized for CHF remains incompletely characterized; particularly in unselected, real-world populations at the national level.
The present study aimed to address this knowledge gap by systematically evaluating the association between AFl and key in-hospital outcomes among patients admitted for CHF. Drawing on a large, unselected cohort derived from nationwide inpatient data in Germany, we sought to generate robust, population-level insights into the clinical relevance of rhythm status in this high-risk group.
Methods
Data Source and Study Population
This retrospective, population-based cohort study aimed to characterize the clinical profiles, therapeutic interventions, complications, and in-hospital outcomes of patients hospitalized for CHF, with a specific focus on differences according to rhythm status - namely, the presence or absence of AFl. To this end, we analyzed nationwide administrative hospital data encompassing all admissions in Germany between 1 January 2014 and 31 December 2022 (Figure: graphical abstract).
The study was based on the German inpatient hospital discharge dataset, compiled as part of the national hospital reimbursement system. Since 2002, all hospitals in Germany are legally required to submit standardized information on each inpatient stay to the Institute for the Hospital Remuneration System (Institut für das Entgeltsystem im Krankenhaus, InEK; Siegburg, Germany; http://www.g-drg.de). These data are made accessible for scientific research through the Research Data Centre (RDC) of the Federal Statistical Office and the Statistical Offices of the Federal States (DESTATIS; https://www.destatis.de; DOI: 10.21242/23141.2014.00.00.6.1.0 to 10.21242/23141.2022.00.00.6.1.0).
The dataset included all inpatient cases from hospital admissions, excluding admissions to psychiatric and psychosomatic units. Analyses were performed at the level of hospitalizations, as the dataset does not include unique patient identifiers. A total of 4,057,291 hospitalizations with a primary diagnosis of CHF - defined using the International Classification of Diseases, 10th Revision, German Modification (ICD-10-GM) codes I50.* - were identified. Patients were stratified by the presence (AFl) (ICD-10-GM code I48.*) or the absence of AFl (non-AFl). Diagnoses and procedures were identified using the ICD-10-GM, and the German procedure classification (Operationen- und Prozedurenschlüssel, OPS; Supplementary Tables S1 and S2). If a code was not recorded during the hospital stay, the corresponding variable was treated as absent.
Analytic scripts were developed and validated using a synthetic dataset structurally equivalent to the original DESTATIS data. As direct access to the raw data was not permitted, all statistical analyses were performed by DESTATIS staff based on our pre-specified scripts. Additional methodological details are available in previous work by our group [8-10].
Baseline characteristics included cardiovascular risk factors (AHT, DM, dyslipidemia, obesity, and nicotine use) and cardiovascular comorbidities (coronary heart disease (CHD), peripheral artery disease (PAD), chronic kidney disease (CKD), ischaemic and haemorrhagic stroke, secondary diagnosis of chronic right and left heart failure (CL/RHF), previous stroke, previous coronary artery bypass grafting (CABG), cerebrovascular disease (CeVD), previous valve replacement, myocardial infarction (MI), and previous percutaneous coronary intervention (PCI)) (Table 1).
Cardiovascular risk profile and comorbidities in CHF hospitalizations, stratified by AFl status.
| AFl | non-AFl | p-value | |
|---|---|---|---|
| 2,307,803 | 1,749,488 | ||
| Sex ♂ | 48.60 (1,121,703) | 50.89 (890,300) | < 0.0001 |
| Cardiovascular risk factors | |||
| DM % (N) | 38.11 (879,480) | 38.43 (672,414) | < 0.0001 |
| dyslipidemia % (N) | 28.32 (653,628) | 28.84 (504,569) | < 0.0001 |
| obesity % (N) | 10.38 (239,524) | 11.58 (202,611) | < 0.0001 |
| nicotine abuse % (N) | 1.21 (28,029) | 2.71 (47,407) | < 0.0001 |
| AHT % (N) | 76.72 (1,770,634) | 73.52 (1,286,198) | < 0.0001 |
| cardiovascular comorbidities | |||
| ischemic stroke % (N) | 0.51 (11,777) | 0.40 (7,049) | < 0.0001 |
| PAD % (N) | 5.74 (132,542) | 5.75 (100,631) | 0.7056 |
| hemorrhagic stroke % (N) | 0.11 (2,595) | 0.08 (1,341) | < 0.0001 |
| CRHF % (N) | 29.03 (669,893) | 23.83 (416,977) | < 0.0001 |
| CLHF % (N) | 25.26 (583,000) | 19.81 (346,497) | < 0.0001 |
| NYHA I % (N) | 0.25 (5,701) | 1.14 (19,997) | < 0.0001 |
| NYHA II % (N) | 2.76 (63,795) | 5.95 (104,123) | < 0.0001 |
| NYHA III % (N) | 25.55 (589,566) | 26.71 (467,346) | < 0.0001 |
| NYHA IV % (N) | 33.64 (776,430) | 33.70 (589,504) | 0.271 |
| NYHA unknown % (N) | 0.35 (8,053) | 0.68 (11,861) | < 0.0001 |
| CKD % (N) | 54.10 (1,248,610) | 44.48 (778,112) | < 0.0001 |
| CHD % (N) | 30.13 (695,322) | 30.71 (537,329) | < 0.0001 |
| previous stroke % (N) | 2.98 (68,803) | 2.51 (43,958) | < 0.0001 |
| previous CABG % (N) | 7.83 (180,749) | 7.34 (128,340) | < 0.0001 |
| CeVD % (N) | 1.22 (28,118) | 1.37 (23,949) | < 0.0001 |
| previous valve % (N) | 2.33 (53,803) | 1.47 (25,803) | < 0.0001 |
| previous MI % (N) | 7.73 (178,379) | 8.90 (155,691) | < 0.0001 |
| previous PCI % (N) | 20.55 (474,168) | 19.98 (244,539) | < 0.0001 |
Cardiovascular risk factors and cardiovascular comorbidities in patients hospitalized due to CHF analyzed according to the presence or absence of AFl. Absolute and relative frequencies. AFl: Atrial flutter/fibrillation, AHT: arterial hypertension, CHF: chronic heart failure, CLHF: chronic left ventricular heart failure, CKD: chronic kidney disease, CRHF: chronic right ventricular heart failure, CeVD: cerebrovascular disease, CHD: coronary heart disease, DM: diabetes mellitus, LV: left ventricular, MI: myocardial infarction, NYHA: New York Heart Association, PAD: peripheral artery disease, PCI: percutaneous coronary intervention.
We also defined procedures indicative of cardiovascular care intensity; left-heart catheterization (LHC), PCI, implantation of drug-eluting or bare-metal stents (DES, BMS), use of drug-eluting balloons (DEB), plain old balloon angioplasty (POBA), and CABG (Supplementary Table S3). Hospital-recorded complications included cardiogenic shock, acute kidney injury (AKI), renal replacement therapy, resuscitation with LV support, mechanical circulatory support (e.g. extracorporeal membrane oxygenation (ECMO), IMPELLA, intra-aortic balloon pump (IABP)), and mechanical ventilation (Figure 1; Supplementary Table S4). Outcomes of interest included the implantation of univentricular or biventricular intracorporeal pumps, total artificial heart replacement, orthotopic or heterotopic heart transplantation (HTx), heart-lung transplantation, and in-hospital mortality (Table 2).
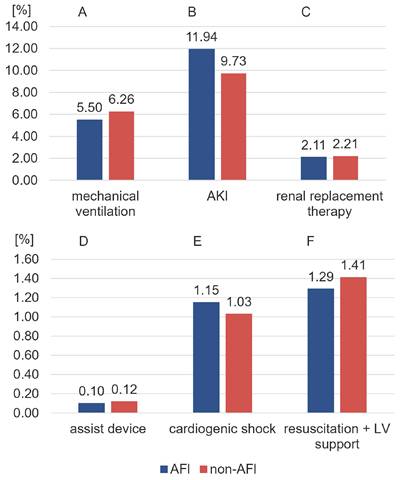
Occurrence of selected complications among patients hospitalized for CHF, stratified by rhythm status. Bar charts compare relative frequencies of mechanical ventilation, AKI, and renal replacement therapy (top panel), as well as assist device, cardiogenic shock and resuscitation with LV support (bottom panel) between patients with AFl (blue) and without AFl (non-AFl; red). AFl: Atrial flutter/fibrillation, AKI: acute kidney injury, CHF: chronic heart failure, LV: left ventricular.
Outcomes in CHF hospitalizations, stratified by AFl status.
| AFl | non-AFl | p-value | |
|---|---|---|---|
| univentricular intracorporeal pump % (N) | 0.08 (1,789) | 0.06 (1,027) | < 0.0001 |
| biventricular intracorporeal pump % (N) | < 0.01 (≤ 2) | < 0.01 (≤ 2) | - |
| total artificial heart % (N) | < 0.01 (11) | < 0.01 (14) | 0.1935 |
| orthotopic HTx % (N) | 0.01 (280) | 0.01 (230) | 0.3669 |
| heterotopic HTx % (N) | 0.00 (0) | 0.00 (0) | - |
| heart-lung-Tx % (N) | < 0.01 (≤ 2) | < 0.01 (≤ 2) | - |
| in-hospital mortality % (N) | 8.30 (191,541) | 8.66 (151,553) | < 0.0001 |
Outcomes in patients hospitalized due to CHF analyzed according to the presence or absence of AFl. Absolute and relative frequencies. AFl: Atrial flutter/fibrillation, CHF: chronic heart failure, HTx: heart transplantation, Tx: transplantation.
Median values for age, length of in-hospital stay, and health care costs were compared between AFl and non-AFl. Cost data were based on the total reimbursements received by hospitals per case from statutory health insurance funds, reflecting the scope of services provided (Supplementary Table S5).
Ethics and Consent
This study was based exclusively on anonymized secondary data from the nationwide German hospital discharge database provided by the Research Data Centre of the Federal Statistical Office (DESTATIS). In accordance with German data protection legislation and institutional regulations, no direct patient contact occurred, and no identifiable individual-level data were accessible to the investigators. Therefore, informed consent was waived, and a priori approval by an institutional ethics committee was not required. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (Br Med J 1964; ii:177).
Individual-level raw data could not be accessed or exported. For all figures, the underlying aggregated numerical values used for statistical analyses and visualizations are provided in the Online Supplement, thereby ensuring transparency and reproducibility within the permitted data protection framework.
Due to the use of nationwide administrative hospital data, residual confounding and coding-related bias cannot be excluded. Moreover, analyses were performed at the level of hospitalizations rather than individual patients, as unique patient identifiers were not available, precluding longitudinal linkage of repeated admissions.
Statistical Analysis
No prospective sample size or power calculation was performed, as this study represents a nationwide census of all hospitalizations fulfilling the predefined inclusion criteria within the study period. Consequently, the sample size was determined by data availability rather than by a priori assumptions, rendering formal sample size calculations not applicable.
To assess differences between AFl and non-AFl, categorical variables were analyzed using the Chi-square test, while continuous variables were evaluated using the Wilcoxon rank-sum test.
Multivariable logistic regression models were used to assess predictors of in-hospital mortality in patients hospitalized with CHF. Separate models were constructed to estimate age-stratified mortality risk in patients with and without AFl, as well as to compare mortality between rhythm groups within each age stratum (Figure 2). A second model included cardiovascular risk factors, comorbidities, and NYHA class to identify independent predictors of in-hospital mortality (Figure 3). Odds ratios and 95% confidence intervals were calculated. The models adjusted for all included covariates simultaneously, with appropriate reference categories (e.g. male sex, absence of comorbidity, NYHA “no CLHF”). Given the exploratory nature of this secondary analysis of administrative data, p-values were interpreted descriptively and not as formal hypothesis testing. This approach aligns with STROBE recommendations for observational studies to avoid overinterpretation of statistical significance.
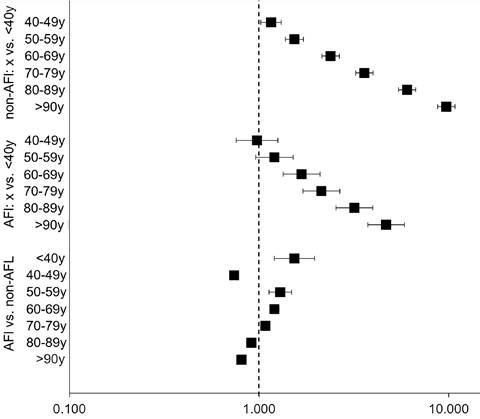
Age-dependent association between AFl status and in-hospital mortality among patients hospitalized with CHF. Forest plot displaying odds ratios (OR) for in-hospital mortality stratified by age and rhythm status. The top and middle panels show the effect of increasing age (reference: <40 years) on in-hospital mortality in non-AFl and AFl patients, respectively. The bottom panel compares the odds of death in AFl versus non-AFl patients within each age stratum. Squares indicate point estimates; horizontal lines represent 95% confidence intervals (Supplementary Table S6). AFl: atrial fibrillation/flutter, CHF: chronic heart failure.
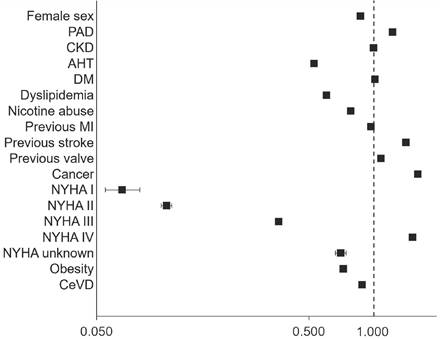
Multivariable predictors of in-hospital mortality among patients hospitalized with CHF. Adjusted odds ratios with 95% confidence intervals are shown for demographic variables, cardiovascular risk factors, comorbidities, and NYHA functional class. The reference category for each binary variable is not shown but includes, for example, male sex, no comorbidity, and “no CLHF” for NYHA comparisons. Variables with ORs > 1 were associated with increased in-hospital mortality; those with ORs < 1 were associated with reduced risk. Squares indicate point estimates; horizontal lines represent 95% confidence intervals (Supplementary Table S7). AHT: Arterial hypertension, CHF: chronic heart failure, CKD: chronic kidney disease, CeVD: cerebrovascular disease, DM: diabetes mellitus, PAD: peripheral artery disease, MI: myocardial infarction, NYHA: New York Heart Association.
P-values were two-sided, and values below 0.05 were considered potentially statistically noticeable. Statistical computations were performed using SAS (version 9.3; SAS Institute Inc., Cary, NC, USA) and R statistical software (version 4.3.2; released 31 October 2023).
Results
Study Population and Baseline Characteristics
Our study included a total of 4,057,291 hospitalizations with a primary diagnosis of CHF (I50.*); 2,307,803 (56.88%) had a diagnosis of AFl. Patients with AFl had a higher median age (82 vs. 79 years) and were more likely to be female (51.40% vs. 49.11%; p < 0.001) (Table 1).
AFl was associated with a higher burden of comorbidities, including CKD (54.10% vs. 44.48%; p < 0.001), AHT (76.72% vs. 73.52%; p < 0.001), CRHF (29.03% vs. 23.83%; p<0.001), and CLHF (25.26% vs. 19.81%; p < 0.001) (Table 1). Furthermore, ischemic and hemorrhagic strokes, prior valve interventions, and previous PCIs or CABG were more prevalent in the AFl group. In contrast, non-AFl patients more frequently had nicotine abuse, DM, CHD, obesity, and a history of previous MI (Table 1).
The distribution across NYHA classes differed between groups, with patients without AFl more frequently classified as NYHA I-III, whereas NYHA IV prevalence was comparable between groups (33.64% vs. 33.70%; p = 0.271) (Table 1).
Non-AFl were more likely to receive invasive cardiac procedures during hospitalization, including LHC, PCI, DES and POBA (Supplementary Table S3). CABG rates were low and comparable between groups (Supplementary Table S3).
In-hospital Outcomes and Complications
AFl was associated with a higher incidence of AKI (11.9% vs. 9.7%; p < 0.001) and cardiogenic shock (1.15% vs. 1.03%; p < 0.001) (Figure 1; Supplementary Table S4). Paradoxically, patients with AFl had lower rates of renal replacement therapy (2.11% vs. 2.21%; p < 0.001) (Figure 1; Supplementary Table S4). They further had lower rates of mechanical ventilation, implantation of assist devices and combined resuscitation with LV support (Figure 1; Supplementary Table S4).
Despite a higher comorbidity burden and age, in-hospital mortality was slightly lower in the AFl group (8.30% vs. 8.66%; p < 0.001) (Table 2). The use of assist devices and organ transplant procedures was rare in both groups, reflecting the advanced age and clinical frailty of the population (Table 2).
Patients with AFl had a longer median hospital stay (8.00 [6.00-13.00] vs. 7.00 [4.00-11.00] days; Supplementary Table S5), potentially due to increased complication rates and comorbidity burden. Median health care costs were comparable between both groups (2,928.96 [2,497.79-3,386.37] € vs. 2,922.67 [2,498.48-3,421.30] €; Supplementary Table S5).
Among CHF patients who underwent mechanical ventilation, the median duration of ventilation was longer in those with AFl compared to those without (28.00 [7.00-91.00] vs. 21.00 [5.00-71.00] hours).
Multivariable Analysis of In-hospital Mortality
In multivariable logistic regression, both age and the presence of AFl were independently associated with higher in-hospital mortality in most age groups (Figure 2, Supplementary Table S6). Among patients with AFl, the odds of death increased steeply across age groups, reaching a maximum in those aged > 90 years.
AFl was associated with lower in-hospital mortality compared to non-AFl in specific age groups, namely 40-49, 80-89, and > 90 years. In all other age strata, the presence of AFl conferred a neutral or slightly elevated mortality risk (Figure 2, Supplementary Table S6).
Several comorbid conditions were independently associated with increased in-hospital mortality, including PAD (OR: 1.24; 95% CI: 1.22-1.27), CKD (OR: 1.10; 95% CI: 1.00-1.20), prior stroke (OR: 1.43; 95% CI: 1.40-1.47), previous valve surgery (OR: 1.31; 95% CI: 1.28-1.35), and cancer (OR: 1.38; 95% CI: 1.34-1.42), all with p-values < 0.0001 (Figure 3, Supplementary Table S7). In contrast, AHT (OR: 0.53; 95% CI: 0.53-0.54), dyslipidemia (OR: 0.60; 95% CI: 0.59-0.60), and nicotine abuse (OR: 0.79; 95% CI: 0.76-0.82) were associated with reduced odds of in-hospital mortality (Figure 3, Supplementary Table S7). Female patients had a lower mortality than males (OR: 0.87; 95% CI: 0.87-0.88; p < 0.0001) (Figure 3, Supplementary Table S7).
NYHA class was strongly predictive of mortality. Patients classified as NYHA class IV had the highest risk (OR: 1.54; 95% CI: 1.52-1.56), whereas those in NYHA I or II had significantly lower odds of death, reflecting less advanced disease (Figure 3, Supplementary Table S7).
Discussion
In this large nationwide cohort of more than four million hospitalizations for CHF, over half of patients were diagnosed with AFl. These patients were older, more often female, and exhibited a markedly higher burden of comorbidities, including CKD, AHT and stroke. Our findings emphasize that AFl in CHF is not merely coincidental arrhythmia but rather a marker of advanced cardiac disease and clinical frailty. We focused on in-hospital outcomes, as nationwide longitudinal follow-up data are not available in Germany, and short-term outcomes remain highly relevant for acute clinical decision making and resource allocation.
Despite their higher age and comorbidity burden, patients with AFl showed slightly lower in-hospital mortality. This seemingly paradoxical finding may reflect earlier presentation, closer monitoring, or differences in clinical management. Importantly, the association between AFl and mortality was age-dependent: AFl was linked to lower mortality in patients aged 40-49, 80-89, and > 90 years, while it conferred neutral or modestly increased risk in other age groups. These findings highlight that the prognostic impact of atrial arrhythmia in CHF is heterogeneous and modulated by age.
Differences in comorbidity profiles between rhythm groups suggest distinct underlying CHF phenotypes. While most previous studies have addressed atrial flutter or atrial fibrillation in highly selected HF populations, large-scale data on the combined burden of atrial fibrillation and flutter remain scarce [11]. In this study, we used “AFl” to collectively refer to atrial fibrillation and/or atrial flutter arrhythmias, reflecting their frequent coexistence and overlapping clinical context in hospitalized CHF patients. The AFl group was enriched for conditions such as AHT and female sex - characteristics typically associated with HF with preserved EF (HFpEF) - while the non-AFl cohort more commonly exhibited nicotine abuse and prior MI, features consistent with a more ischemic phenotype. Unfortunately, due to data limitations, EF could not be assessed.
The observed differences in comorbidity profiles between AFl and non-AFl patients raise the possibility that distinct therapeutic responses may exist across HF phenotypes.
Emerging evidence indicates that contemporary HF therapies may influence outcomes irrespective of rhythm status [12-15]. Subgroup analyses from large, randomized trials have demonstrated consistent benefits of sodium-glucose cotransporter 2 (SGLT2) inhibitors in patients with and without atrial arrhythmia, while early data suggest potential rhythm-modifying effects of glucagon-like peptide-1 (GLP-1) receptor agonists [13-15]. In addition, guideline-recommended CHF therapies such as beta-blockers overlap substantially with pharmacological rate control strategies for AFl, underscoring the close pathophysiological and therapeutic interplay between both conditions [16].
In our cohort, patients with AFl underwent fewer invasive cardiac procedures but experienced longer hospital stays despite comparable costs, suggesting a more prolonged yet less intervention-intensive in-hospital course. Whether this reflects appropriate treatment individualization in older or frailer patients or an underuse of evidence-based interventions remains unclear. Randomized trials such as CASTLE-AF have demonstrated improved outcomes with catheter ablation in selected CHF patients, highlighting the importance of individualized rhythm management strategies [17]. Although EF and ablation status were not available in our dataset, the observed variation in mortality by rhythm status and age may partly reflect underlying differences in rhythm management strategies. In younger patients, for example, the lower in-hospital mortality associated with AFl could suggest earlier or more targeted rhythm control, aligning with the paradigm supported by CASTLE-AF [17]. While this may represent appropriate tailoring of care in frailer individuals, it could also indicate underutilization of evidence-based interventions in selected candidates.
In multivariable modelling, classical predictors of mortality - age, NYHA class, CKD, PAD, stroke, and cancer - remained prominent. Yet, AHT, dyslipidemia, and nicotine abuse were inversely associated with mortality, possibly reflecting survivorship bias or unmeasured confounding. Our findings raise the hypothesis that the prognostic impact of AFl is not uniform but dynamically modulated by age and comorbidity burden. Beyond rhythm status alone, integrated clinical risk assessment may further improve prognostic stratification in CHF populations. In this context, the CHA₂DS₂-VASc score - originally developed for thromboembolic risk estimation in AFl - has also been associated with mortality and adverse cardiovascular outcomes in CHF patients irrespective of atrial arrhythmia status. Recent studies demonstrated that increasing CHA₂DS₂-VASc scores correlate with higher mortality and rehospitalization rates even in CHF patients without AFl, likely reflecting the cumulative impact of age, vascular disease, and comorbidity burden [18,19]. This concept is consistent with our findings, in which age, NYHA class, CKD, PAD, stroke, and other comorbidities appeared as important determinants of in-hospital mortality independent of rhythm status, further stressing the importance of comprehensive risk assessment beyond the presence or absence of atrial arrhythmia alone. The paradoxical survival advantage seen in the youngest and oldest strata may stem from more regular follow-up, selective survival, or other unmeasured protective factors.
Limitations
This study has several limitations that warrant consideration. First, it is based on administrative data from a national inpatient registry, which - although comprehensive in scope - lacks clinical granularity. Parameters such as left ventricular ejection fraction, biomarker levels, medical therapy, rhythm type and duration (paroxysmal, persistent, or permanent), and ablation status were not available, limiting our ability to stratify patients by CHF phenotype, arrhythmia characteristics, or therapeutic intensity. Second, the analysis was performed at the level of hospitalizations rather than unique patients, as the dataset does not contain individual patient identifiers. Consequently, multiple admissions of the same patient could not be linked, potentially leading to overrepresentation of frequently hospitalized individuals, although this approach reflects the real-world burden on the health care system. Third, the observational design precludes causal inference; residual confounding from unmeasured factors such as frailty, socioeconomic status, or physician decision-making is likely, and treatment allocation during hospitalization may have been influenced by these factors. The lack of information on antiarrhythmic or other cardiovascular medications further limits adjustment for treatment effects. Fourth, atrial fibrillation and atrial flutter were combined under the term “AFl” because the ICD-10-GM coding in the nationwide dataset does not reliably distinguish between these arrhythmias. While they frequently coexist and share overlapping risk factors and management strategies in CHF, they may differ in pathophysiology, prognosis, and optimal treatment - representing a major limitation of this study. Fifth, the descriptive interpretation of p-values reflects the exploratory nature of the analysis and aims to emphasize effect sizes and clinical relevance rather than formal statistical significance. Finally, only in-hospital outcomes were assessed; long-term endpoints such as post-discharge mortality, rehospitalization, or quality of life could not be evaluated, precluding conclusions on the sustained impact of rhythm status beyond the index hospitalization.
Supplementary Material
Supplementary tables.
Declaration of Generative AI and AI-assisted Technologies in the Manuscript Preparation Process
During the preparation of this manuscript, the authors used ChatGPT (OpenAI) to support language editing and improve clarity and structure of the text. All content was critically reviewed and edited by the authors, who take full responsibility for the final version of the manuscript.
Data Availability
The data underlying this article are available from the Research Data Centre of the Federal Statistical Office (DESTATIS, Germany) under strict data protection conditions and cannot be shared publicly.
Competing Interests
HR reports personal fees from Daiichi Sankyo, Pfizer, MedUpdate, StreamedUp, DiaPlan, NeoVasc, Pluristem, NovoNordisk and Corvia. WAL reports personal fees and research support from Merck, Sharp, and Dohme as well as Dewpoint Therapeutics. Furthermore, institutional grants were received from Pluristem, BMS, Pfizer, Bard and Biotronik. JRS reports personal fees from Abbott, Boehringer Ingelheim, BMS and Novartis. AJH and JF have nothing to declare.
References
1. Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of Atrial Fibrillation in the 21st Century: Novel Methods and New Insights. Circ Res. 2020;127:4-20 doi: 10.1161/CIRCRESAHA
2. Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. 2016;13:368-78 doi: 10.1038/nrcardio.2016.25
3. Darvish M, Shakoor A, Feyz L, Schaap J, van Mieghem NM, de Boer RA. et al. Heart failure: assessment of the global economic burden. Eur Heart J. 2025;46:3069-3078 doi: 10.1093/eurheartj/ehaf323
4. Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS. et al. Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association. Circulation. 2022;145:e153-e639 doi: 10.1161/CIR.0000000000001052. [Epub ahead of print]
5. Carlisle MA, Fudim M, DeVore AD, Piccini JP. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019;7:447-456 doi: 10.1016/j.jchf.2019.03.005
6. Newman JD, O'Meara E, Böhm M, Savarese G, Kelly PR, Vardeny O. et al. Implications of Atrial Fibrillation for Guideline-Directed Therapy in Patients with Heart Failure: JACC State-of-the-Art Review. J Am Coll Cardiol. 2024;83:932-950 doi: 10.1016/j.jacc.2023.12.033
7. Sartipy U, Dahlström U, Fu M, Lund LH. Atrial Fibrillation in Heart Failure with Preserved, Mid-Range, and Reduced Ejection Fraction. JACC Heart Fail. 2017;5:565-574 doi: 10.1016/j.jchf.2017.05.001
8. Freisinger E, Fuerstenberg T, Malyar NM, Wellmann J, Keil U, Breithardt G. et al. German nationwide data on current trends and management of acute myocardial infarction: discrepancies between trials and real-life. Eur Heart J. 2014;35:979-88 doi: 10.1093/eurheartj/ehu043
9. Kuehnemund L, Koeppe J, Feld J, Wiederhold A, Illner J, Makowski L. et al. Gender differences in acute myocardial infarction-A nationwide German real-life analysis from 2014 to 2017. Clin Cardiol. 2021;44:890-898 doi: 10.1002/clc.23662
10. Hobbach AJ, Feld J, Sindermann JR, Reinecke H. Evolving trends and persistent challenges in chronic left ventricular heart failure management: insights from a 9-year analysis of in-hospital outcomes in Germany. Clin Res Cardiol. 2025 doi: 10.1007/s00392-025-02679-4. [Epub ahead of print]
11. Diamant MJ, Andrade JG, Virani SA, Jhund PS, Petrie MC, Hawkins NM. Heart failure and atrial flutter: a systematic review of current knowledge and practices. ESC Heart Fail. 2021;8:4484-4496 doi: 10.1002/ehf2.13526
12. Oraii A, Healey JS, Kowalik K, Pandey AK, Benz AP, Wong JA. et al. Mineralocorticoid receptor antagonists and atrial fibrillation: a meta-analysis of clinical trials. Eur Heart J. 2024;45:756-774 doi: 10.1093/eurheartj/ehad811
13. Pandey AK, Okaj I, Kaur H, Belley-Cote EP, Wang J, Oraii A. et al. Sodium-Glucose Co-Transporter Inhibitors and Atrial Fibrillation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Am Heart Assoc. 2021;10:e022222 doi: 10.1161/JAHA
14. Butt JH, Docherty KF, Jhund PS, de Boer RA, Böhm M, Desai AS. et al. Dapagliflozin and atrial fibrillation in heart failure with reduced ejection fraction: insights from DAPA-HF. Eur J Heart Fail. 2022;24:513-525 doi: 10.1002/ejhf.2381
15. Sundaram V. TRANSFORM-AF: targeting metabolic therapy with GLP-1 receptor agonism for secondary prevention in atrial fibrillation. Presented at: HRS 2025. April 25. 2025 San Diego, CA
16. Van Gelder IC, Rienstra M, Bunting KV, Casado-Arroyo R, Caso V, Crijns HJGM. et al. ESC Scientific Document Group. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45:3314-3414 doi: 10.1093/eurheartj/ehae176
17. Marrouche NF, Brachmann J, Andresen D, Siebels J, Boersma L, Jordaens L. et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N Engl J Med. 2018;378:417-427 doi: 10.1056/NEJMoa1707855
18. Shuvy M, Zwas DR, Keren A, Gotsman I. Value of the CHA2DS2-VASc score for predicting outcome in patients with heart failure. ESC Heart Fail. 2020;7:2553-2560 doi: 10.1002/ehf2.12831
19. Sonaglioni A, Lonati C, Rigamonti E, Viganò M, Nicolosi GL, Proietti M. et al. CHA2DS2-VASc score stratifies mortality risk in heart failure patients aged 75 years and older with and without atrial fibrillation. Aging Clin Exp Res. 2022;34:1707-1720 doi: 10.1007/s40520-022-02107-x
Author contact
![]() Corresponding author: Anastasia J. Hobbach, 1Department of Cardiology I, Coronary, Peripheral Vascular Disease and Heart Failure, University Hospital Münster, Albert-Schweizer Campus 1, 48149 Münster, Germany, ORCID: 0000-0001-6421-8429, Tel: +49 251 83 44234, Email: Anastasia.Hobbachde.
Corresponding author: Anastasia J. Hobbach, 1Department of Cardiology I, Coronary, Peripheral Vascular Disease and Heart Failure, University Hospital Münster, Albert-Schweizer Campus 1, 48149 Münster, Germany, ORCID: 0000-0001-6421-8429, Tel: +49 251 83 44234, Email: Anastasia.Hobbachde.