Impact Factor ISSN: 1449-1907
- Issue 9; 2026
- Issue 8; 2026
- Issue 7; 2026
- Issue 6; 2026
- Issue 5; 2026
- Volume 23; 2026
- Past Issues
- Editorial Board
- Cover Images
- Index & Coverage
- Cover Suggestion
- Special Issues
Introduction
Methods
Results
Discussion
Conclusion
Abbreviations
Supplementary Material
Acknowledgements
References

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2026; 23(8):2511-2523. doi:10.7150/ijms.131673 This issue Cite
Research Paper
Exploratory Immunophenotyping of Programmed cell death-1 (PD-1) Expression and Regulatory T-Cell (Treg) Profiles in Systemic Lupus Erythematosus and Healthy Controls: A Cohort Study with Illustrative Clinical Cases
Po-Jen Hsiao1,2,3, Jeng-Wei Lu4,5,6, Yi-Jung Ho7,8, Shan-Wen Lui9, Ting-Yu Hsieh10, Wun-Long Jheng11,12, Anna Blyzniuk13, Feng-Cheng Liu14 ![]()
1. Division of Nephrology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan, R.O.C.
2. Division of Nephrology, Department of Internal Medicine, Taoyuan Armed Forces General Hospital, Taoyuan, Taiwan, R.O.C.
3. Department of Life Sciences, National Central University, Taoyuan, Taiwan, R.O.C.
4. Department of Bioscience and Biotechnology, National Taiwan Ocean University, Keelung, Taiwan, R.O.C.
5. Biotech Research and Innovation Centre, University of Copenhagen, Copenhagen, Denmark.
6. The Finsen Laboratory, Rigshospitalet/National University Hospital, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
7. School of Pharmacy, National Defense Medical University, Taipei, Taiwan, R.O.C.
8. Graduate Institute of Life Sciences, National Defense Medical University, Taipei, Taiwan, R.O.C.
9. Department of Internal Medicine, Linkou Chang-Gung Memorial Hospital, Taoyuan, Taiwan, R.O.C.
10. Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan, R.O.C.
11. Cancer Center, Hualien Tzu-Chi Hospital, Hualien, Taiwan, R.O.C.
12. Department of Engineering Medicine, Shizuoka Center for Molecular Intelligence, Hamamatsu, Shizuoka, Japan.
13. School of Medicine, O.O. Bogomolets National Medical University, Kyiv, Ukraine.
14. Rheumatology/Immunology and Allergy, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan, R.O.C.
Received 2026-1-18; Accepted 2026-6-4; Published 2026-6-17
Abstract

Background: Immune checkpoint signaling and regulatory T cells (Tregs) play essential roles in immune homeostasis and immune dysregulation in autoimmune diseases. Programmed cell death-1 (PD-1) signaling and Treg dysfunction have been implicated in systemic lupus erythematosus (SLE); however, temporal variation in immune regulatory profiles across disease states remains incompletely characterized. This study aimed to characterize PD-1 expression and Treg-associated immune profiles in patients with SLE compared with healthy controls while descriptively exploring selected illustrative clinical immune contexts.
Methods: An exploratory longitudinal immunophenotyping study was conducted using multiparameter flow cytometry. The primary exploratory cohort included healthy Taiwanese controls (n = 20) and patients with SLE (n = 10). PD-1 expression across representative T-cell subsets and distributions of Treg-associated immune populations were assessed. Where available, paired longitudinal samples obtained during clinically active and stable disease states were evaluated descriptively to characterize temporal immune variation. Additional illustrative clinical cases representing infection-related and postoperative inflammatory conditions were retained separately for contextual interpretation. Because of the exploratory design and modest sample size, all statistical analyses were considered exploratory and hypothesis-generating.
Results: Compared with healthy controls, patients with SLE demonstrated broader inter-individual variation in PD-1 expression and Treg-associated immune profiles, including differences in activated and memory-associated Treg phenotypes. Paired longitudinal evaluation suggested temporal immune variation between clinically active and stable disease states in selected individuals, although substantial heterogeneity remained evident across patients. Healthy controls also demonstrated measurable baseline variability in immune marker distributions. Selected illustrative clinical cases demonstrated heterogeneous checkpoint-associated and regulatory immune profiles under infection-related and postoperative inflammatory conditions.
Conclusion: This exploratory longitudinal immunophenotyping study describes variation in PD-1 expression and Treg-associated immune profiles across healthy individuals and patients with SLE while providing descriptive contextual observations under selected inflammatory and postoperative clinical conditions. Because of the exploratory design, modest cohort size, clinical heterogeneity, and absence of functional immune validation, all findings should be interpreted cautiously and considered exploratory and hypothesis-generating rather than confirmatory. Larger longitudinal studies incorporating standardized immune monitoring and functional immune assessment are warranted to clarify the biological and clinical relevance of these preliminary observations.
Introduction
Immune regulation plays a central role in maintaining host defense, immune tolerance, and tissue homeostasis. Among the key mechanisms governing immune balance, the programmed cell death-1 (PD-1) immune checkpoint functions as a critical inhibitory receptor that modulates T-cell activation and contributes to T-cell exhaustion during chronic immune stimulation [1,2]. The PD-1/PD-L1 axis has also been recognized as an important mediator of immune regulation and a major therapeutic target in cancer and immune-mediated diseases [3]. In parallel, regulatory T cells (Tregs) represent a fundamental component of immune homeostasis. Early studies demonstrated that CD4⁺CD25⁺ T cells are essential for maintaining self-tolerance [4], and subsequent work identified FoxP3 as a master regulator of Treg development and function [5-7]. Together, PD-1 signaling and Treg-mediated suppression constitute interconnected regulatory systems that fine-tune immune responses under both physiological and pathological conditions.
Substantial inter-individual variability in immune responses has been well documented. Population-based studies have shown that immune system composition and responsiveness are influenced by genetic background and environmental exposures, resulting in heterogeneity in immune phenotypes [8-10]. In addition, immune regulatory pathways are highly dynamic and responsive to inflammatory and physiological conditions. Clinical and experimental studies have demonstrated descriptive and hypothesis-generating insight into immune regulatory variation across autoimmune and inflammatory conditions [11-16]. These observations suggest that PD-1 signaling and Treg-associated immune regulation are dynamic and context-dependent rather than fixed immune characteristics [17-20].
Among autoimmune diseases, systemic lupus erythematosus (SLE) is characterized by profound immune dysregulation involving aberrant T-cell activation, defective immune tolerance, and chronic systemic inflammation. Previous studies have suggested that alterations in PD-1 signaling may contribute to immune dysregulation in SLE, while impaired Treg number or function has been implicated in the loss of self-tolerance and disease progression [21-23]. Dysregulation of immune checkpoint pathways may reflect both persistent immune activation and compensatory inhibitory responses, highlighting the potential importance of PD-1 and Treg-associated pathways in disease activity and immune variation. However, despite increasing evidence supporting their biological relevance, temporal variation in PD-1 expression and Treg-associated immune profiles across disease states in SLE remains incompletely characterized. Translating these mechanistic insights into clinical practice requires real-world immunophenotyping data that capture the temporal dynamics of PD-1 and Treg-associated immune profiles across disease states in living patients. Despite accumulating experimental and mechanistic evidence, prospective longitudinal immune profiling studies involving clinically well-characterized SLE cohorts remain limited, particularly in East Asian populations. Bridging this translational gap between laboratory immunology and bedside immune monitoring therefore represents an important motivation for the present study.
To address this gap, we conducted an exploratory longitudinal immunophenotyping study using multiparameter flow cytometry to characterize PD-1 expression and regulatory T-cell-associated immune profiles in patients with SLE compared with healthy controls. Where available, paired longitudinal samples obtained during clinically active and stable disease states were evaluated descriptively to explore temporal immune variation. Selected illustrative clinical cases involving infection-related and postoperative inflammatory conditions were retained separately to provide contextual insight into immune heterogeneity under physiological stress. Given the exploratory nature, modest sample size, and clinical heterogeneity of the study population, all findings are intended to provide descriptive and hypothesis-generating insights rather than support causal or population-level inference, thereby informing future larger and longitudinal investigations.
Methods
Study Cohort and Recruitment Strategy
This study was designed as an exploratory longitudinal immunophenotyping analysis to characterize PD-1 expression and Treg-associated immune profiles in patients with SLE compared with healthy reference controls, while descriptively evaluating immune variation across selected clinical contexts. Participants were recruited using a convenience sampling strategy from clinical and institutional settings. The primary exploratory cohort comprised healthy Taiwanese controls and patients with SLE.
Healthy controls (n = 20) were included to provide reference distributions for baseline immune variability. Healthy participants were defined by the absence of acute or chronic inflammatory disease, no recent infection or surgery within 4 weeks, and no use of immunomodulatory or immunosuppressive medications. The SLE cohort included 10 patients fulfilling the 2019 European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) classification criteria for SLE. The paired blood samples obtained during clinically active disease and stable follow-up were evaluated descriptively to explore temporal immune variation within individuals. Among patients with paired longitudinal follow-up, clinical disease activity generally decreased during stable follow-up relative to clinically active disease states. SLEDAI-2K (Systemic Lupus Erythematosus Disease Activity Index 2000) is a validated composite disease activity index in which higher scores indicate greater lupus disease activity, whereas BILAG (British Isles Lupus Assessment Group disease activity index) evaluates organ-specific disease activity according to the physician's intention to treat [24]. Where available, paired longitudinal blood samples were obtained during clinically active disease and stable follow-up states, with a median sampling interval of 3.5 months (IQR, 2.0-6.0 months). Relevant clinical variables—including comorbidities, treatment exposure, inflammatory markers, disease duration, disease activity, and lupus nephritis status where applicable—were reviewed to provide clinical context for interpretation.
In addition to the primary exploratory cohort, selected individual clinical cases were retained descriptively as illustrative inflammatory and postoperative immune contexts rather than analytical groups. These included a recovery-phase cellulitis case following surgical debridement and a postoperative case following osteoporotic vertebral compression fracture surgery. These illustrative cases were included solely to provide contextual examples of immune variation and were not incorporated into cohort-level statistical analyses. An additional healthy non-Taiwanese participant of Ukrainian (Caucasian) background was evaluated separately in supplementary analyses to illustrate inter-individual immune variability under non-stressed conditions. This participant was not included in the primary exploratory cohort and was not incorporated into formal statistical comparisons or inferential analyses.
Study Design and Analytical Framework
An exploratory longitudinal immunophenotyping approach was adopted. The primary objective was to characterize variation in PD-1 expression and Treg-associated immune profiles in patients with SLE compared with healthy controls and to descriptively evaluate temporal immune variation where paired follow-up data were available. Multiparameter flow cytometry was used to assess representative T-cell, Treg-associated, and B-cell populations across the exploratory cohort.
Representative immune markers were selected to evaluate immune checkpoint activity, regulatory immune pathways, and adaptive immune variation relevant to autoimmune immune dysregulation. PD-1 and exhaustion-related markers were included to assess checkpoint-associated immune activity and T-cell differentiation states, whereas Treg-associated markers were used to characterize regulatory immune populations involved in immune tolerance. Representative B-cell markers were additionally incorporated to provide broader contextual assessment of adaptive immune variation.
Because of the exploratory design and modest sample size, the study was not intended to establish causal relationships, define disease-specific immune signatures, or support population-level inference. Instead, all findings are intended to provide descriptive and hypothesis-generating insight into immune regulatory variation across autoimmune disease and selected inflammatory or postoperative contexts [25,26].
Immune marker distributions were interpreted primarily using individual-level visualization approaches, including dot plots, paired longitudinal displays, and integrated heatmap analyses, to preserve inter-individual variability and avoid overinterpretation of summary immune profiles. Selected illustrative clinical cases and supplementary descriptive observations were evaluated separately from the primary exploratory cohort and were not incorporated into inferential cohort-level analyses.
Flow Cytometry-Based Immunophenotyping
Peripheral venous blood samples were collected in EDTA-containing tubes and processed within 2-4 hours after collection. Peripheral blood mononuclear cells (PBMCs) were isolated using Ficoll-Paque PLUS (GE Healthcare, Uppsala, Sweden), washed, and resuspended in staining buffer for multiparameter flow cytometric analysis.
The gating strategy followed a sequential workflow. Debris and doublets were excluded based on forward and side scatter characteristics, followed by exclusion of non-viable cells using a fixable viability dye. CD3⁺ T cells were identified and subdivided into CD4⁺ and CD8⁺ populations. Regulatory T cells were defined as CD4⁺CD25^highCD127^low/-FoxP3⁺ cells. Treg subsets, including naïve, activated, memory, resting, CD39⁺, Helios⁺, and Tr1-associated populations, were further characterized according to previously established phenotypic definitions and gating strategies [27-31]. B-cell subsets were identified within CD19⁺ cells and classified into naïve, switched memory, transitional, plasmablast, and regulatory B-cell populations based on CD27 and IgD expression [32]. PD-1, KLRG1, Fas, and Tim-3 expression were evaluated across representative T-cell subsets.
Cells were stained with fluorochrome-conjugated monoclonal antibodies targeting representative T-cell, Treg, and B-cell-associated immune markers, including CD3, CD4, CD8, CD25, CD127, PD-1, KLRG1, Fas, Tim-3, CD19, CD27, and IgD. Intracellular FoxP3 staining was performed using a transcription factor staining buffer set according to the manufacturer's instructions. Detailed antibody information and fluorochrome combinations are provided in Supplementary Table S1.
Data acquisition was performed using multicolor flow cytometers (BD FACSCanto II or BD LSRFortessa; BD Biosciences, San Jose, CA, USA), and analyses were conducted using FlowJo software (Tree Star Inc., Ashland, OR, USA). Instrument settings were standardized across samples. Compensation was performed using single-stained controls, and fluorescence-minus-one (FMO) controls were applied for selected markers, including PD-1 and Treg-associated immune markers.
Additional immune markers associated with T-cell activation, differentiation, exhaustion, and senescence—including KLRG1, Fas, and Tim-3—were evaluated according to prior studies of immune checkpoint signaling and T-cell dysfunction [33-35]. Because of the exploratory design and modest cohort size, all immunophenotypic findings were interpreted descriptively and considered hypothesis-generating rather than confirmatory.
Data Interpretation and Visualization
Immune marker distributions were summarized primarily as proportions and visualized using individual-level dot plots, paired longitudinal plots, and integrated heatmaps. Paired longitudinal visualization was used to descriptively illustrate temporal immune variation between clinically active disease and stable follow-up states in patients with SLE where paired samples were available. Individual-level visualization approaches were prioritized to preserve inter-individual variability and avoid overinterpretation of summarized immune distributions within the modest exploratory cohort.
For heatmap visualization, immune marker data were normalized using row-wise z-score transformation across participants included in the primary exploratory cohort, including healthy controls and patients with SLE. Heatmaps were generated solely for descriptive visualization of immune heterogeneity across representative PD-1-associated, Treg-associated, and B-cell immune markers. Because normalization was performed across the full cohort, values represent relative positioning within the study population rather than within-group variation. Given the exploratory design, modest sample size, and clinical heterogeneity of the cohort, heatmap analyses were intended for descriptive pattern recognition only and should not be interpreted as evidence of disease-specific, mechanistic, statistical, or inferential immune differences.
Selected illustrative clinical cases and supplementary descriptive observations were visualized separately from the primary exploratory cohort and interpreted descriptively to provide contextual examples of immune variation under inflammatory and non-inflammatory conditions. These supplementary observations were not incorporated into primary cohort-level interpretation.
Statistical Analysis
Because of the exploratory nature of the study and modest sample size, statistical analyses were performed using non-parametric methods. Continuous variables were summarized primarily as median with interquartile range (IQR). Mean ± standard deviation (SD) values were additionally provided for selected descriptive visualization where appropriate.
Exploratory comparisons between healthy controls and patients with SLE were performed using the Mann-Whitney U test. For participants with paired longitudinal follow-up data, within-individual comparisons between clinically active disease and stable follow-up states were evaluated using the Wilcoxon signed-rank test. Where applicable, descriptive associations between representative immune markers and clinical disease activity variables were explored using Spearman's rank correlation coefficient.
Given the exploratory design, modest cohort size, clinical heterogeneity, and absence of functional immune validation, all statistical findings should be interpreted cautiously and considered hypothesis-generating rather than confirmatory. No formal power calculation or adjustment for multiple comparisons was performed.
Results
Study Cohort and Clinical Characteristics
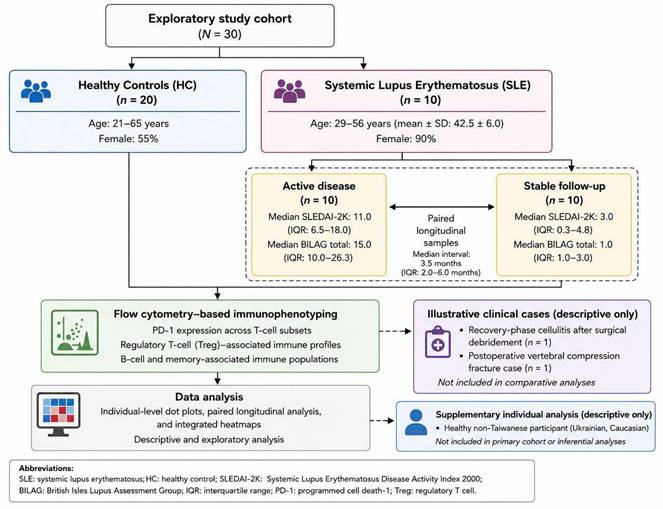
A total of 30 participants were included in the primary exploratory cohort, comprising healthy controls (n = 20) and patients with SLE (n = 10) (Figure 1). The SLE cohort consisted predominantly of female participants (90%) with a mean age of 42.5 ± 6.0 years and a median disease duration of 4.2 years (IQR, 2.1-10.6). Where available, paired longitudinal blood samples were obtained during clinically active disease and stable follow-up states, with a median sampling interval of 3.5 months (IQR, 2.0-6.0 months). Among patients with paired longitudinal follow-up, clinical disease activity decreased during stable follow-up compared with clinically active disease states, as reflected by reductions in both SLEDAI-2K and BILAG scores. Detailed demographic characteristics, disease manifestations, treatment exposure, and longitudinal disease activity data are summarized in Table 1.
Study cohort and analytical framework of the exploratory longitudinal immunophenotyping study. Overview of participant recruitment, cohort composition, longitudinal sampling strategy, and analytical workflow used to characterize immune regulatory profiles in patients with systemic lupus erythematosus (SLE) and healthy controls (HC). The primary exploratory cohort comprised healthy controls (HC, n = 20) and patients with SLE (n = 10), with paired longitudinal follow-up samples obtained during clinically active disease and stable follow-up where available. Clinical variables—including demographics, treatment exposure, inflammatory markers, disease duration, disease activity, lupus nephritis status, and comorbidities—were reviewed for contextual interpretation. Two selected individual clinical cases (n = 2), representing post-infectious recovery and postoperative inflammatory conditions, were retained separately for descriptive contextual visualization and were not included in cohort-level statistical comparisons. Peripheral blood mononuclear cells (PBMCs) were analyzed using multiparameter flow cytometry to assess programmed cell death-1 (PD-1) expression across representative T-cell subsets and regulatory T-cell (Treg)-associated immune profiles. Analytical approaches included descriptive immune profiling, exploratory non-parametric analyses, paired longitudinal visualization, and integrated heatmap analyses to preserve inter-individual immune variability. Findings are intended to provide descriptive and hypothesis-generating insights rather than causal or population-level inference. Abbreviations: HC, healthy controls; SLE, systemic lupus erythematosus; PBMC, peripheral blood mononuclear cell; PD-1, programmed cell death-1; Treg, regulatory T cell; EULAR/ACR, European League Against Rheumatism/American College of Rheumatology; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index.
Baseline demographic and clinical characteristics of patients with systemic lupus erythematosus
| Variable | SLE cohort (n = 10) |
|---|---|
| Sex, female, n (%) | 9 (90) |
| Age, years | 42.5 ± 6.0 |
| Disease duration, years | 4.2 (2.1-10.6) |
| Lupus nephritis, n (%) | 3 (30) |
| Pulmonary arterial hypertension, n (%) | 2 (20) |
| Sjögren syndrome/interstitial lung disease, n (%) | 1 (10) |
| Cerebrovascular involvement with suspected antiphospholipid syndrome, n (%) | 1 (10) |
| Opportunistic infection history, n (%) | 1 (10) |
| Corticosteroid treatment, n (%) | 10 (100) |
| Immunosuppressive treatment, n (%) | 8 (80) |
| Hydroxychloroquine treatment, n (%) | 7 (70) |
| SLEDAI-2K score during active disease | 11.0 (6.5-18.0) |
| SLEDAI-2K score during stable follow-up | 3.0 (0.3-4.8) |
| BILAG total score during active disease | 15.0 (10.0-26.3) |
| BILAG total score during stable follow-up | 1.0 (1.0-3.0) |
Abbreviations: SLE, systemic lupus erythematosus; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000; BILAG, British Isles Lupus Assessment Group; APS, antiphospholipid syndrome.
Data presentation: Data are presented as mean ± standard deviation (SD), median (interquartile range [IQR]), or number (%), as appropriate. Immunosuppressive agents included mycophenolate mofetil, azathioprine, tacrolimus, and cyclophosphamide according to individual clinical indications.
Comprehensive flow cytometry-based immunophenotyping focused on PD-1 expression across representative T-cell subsets and the distribution of Treg-associated immune populations. Immune marker distributions were visualized primarily using individual-level dot plots, paired longitudinal displays, and integrated heatmaps because of the exploratory design and modest cohort size.
Baseline Immune Variability in Healthy Controls
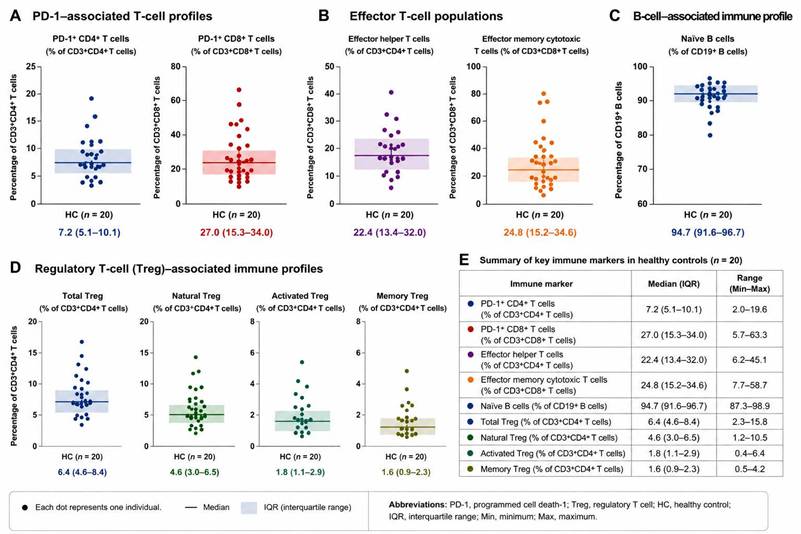
Among healthy controls, PD-1 expression and Treg-associated immune profiles demonstrated measurable inter-individual variability across multiple immune markers (Figure 2). Effector helper and effector memory cytotoxic T-cell populations showed moderate variation across participants, whereas naïve B-cell populations remained relatively preserved in most individuals. Regulatory T-cell subsets also demonstrated variability, particularly among activated and memory-associated Treg populations, while overall checkpoint-associated and regulatory immune profiles remained relatively stable within healthy reference distributions. These observations provided contextual baseline immune variability for exploratory comparison with patients with SLE.
Baseline immune reference distributions in healthy controls. Individual-level distributions of key immune markers in healthy controls (HC, n = 20) were evaluated using flow cytometry-based immunophenotyping. Each dot represents one individual participant. Horizontal lines indicate the median, and shaded areas represent the interquartile range (IQR). (A) PD-1-associated T-cell profiles, including PD-1⁺ CD4⁺ T cells and PD-1⁺ CD8⁺ T cells. (B) Effector T-cell populations, including effector helper T cells and effector memory cytotoxic T cells. (C) B-cell-associated immune profile showing naïve B-cell distribution. (D) Regulatory T-cell (Treg)-associated immune profiles, including total Treg, natural Treg, activated Treg, and memory Treg populations. (E) Summary table showing median values, interquartile ranges, and overall ranges for the evaluated immune markers in healthy controls. These analyses were performed to establish reference distributions and illustrate baseline inter-individual immune variability under non-inflammatory conditions. Abbreviations: PD-1, programmed cell death-1; Treg, regulatory T cell; HC, healthy control; IQR, interquartile range.
PD-1 Expression in SLE and Longitudinal Immune Variation
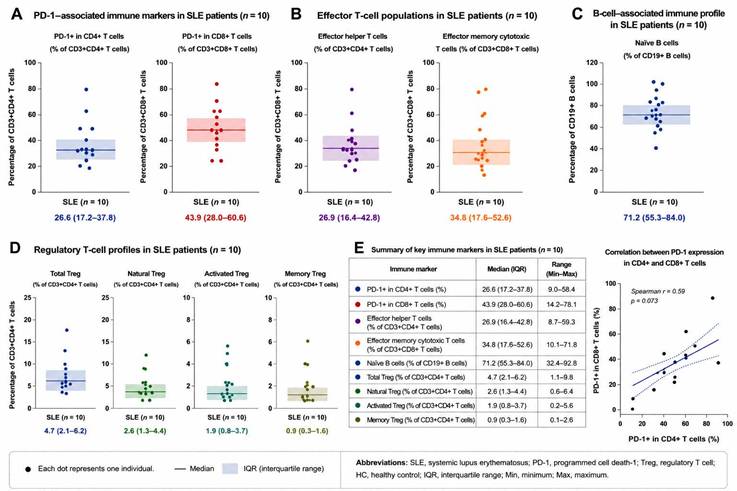
Patients with SLE demonstrated broader heterogeneity across PD-1-associated immune markers compared with healthy controls. Naïve B-cell distributions also appeared lower and more heterogeneous in several patients with SLE compared with healthy controls (Figure 3). Relative increases in PD-1-associated immune phenotypes were observed in selected patients during clinically active disease states, particularly within effector helper and cytotoxic T-cell populations. Where paired longitudinal samples were available, temporal variation in immune checkpoint-associated profiles were observed between active disease and stable follow-up. In several individuals, reductions in selected PD-1-associated immune markers coincided with lower SLEDAI-2K and BILAG disease activity scores during stable follow-up, although substantial inter-individual variability remained evident.
Immune profiling of patients with systemic lupus erythematosus. Individual-level distributions of key immune markers in patients with systemic lupus erythematosus (SLE, n = 10) were evaluated using flow cytometry-based immunophenotyping. Each dot represents one individual participant. Horizontal lines indicate the median, and shaded areas represent the interquartile range (IQR). (A) PD-1-associated immune markers, including PD-1⁺ CD4⁺ T cells and PD-1⁺ CD8⁺ T cells. (B) Effector T-cell populations, including effector helper T cells and effector memory cytotoxic T cells. (C) B-cell-associated immune profile showing naïve B-cell distribution. (D) Regulatory T-cell (Treg)-associated immune profiles, including total Treg, natural Treg, activated Treg, and memory Treg populations. (E) Summary table showing median values, interquartile ranges, and overall ranges for the evaluated immune markers in patients with SLE. The correlation plot demonstrates the relationship between PD-1 expression in CD4⁺ and CD8⁺ T cells using Spearman correlation analysis. These analyses were performed to characterize inter-individual immune heterogeneity and exploratory immune checkpoint-associated alterations in patients with SLE. Abbreviations: SLE, systemic lupus erythematosus; PD-1, programmed cell death-1; Treg, regulatory T cell; HC, healthy control; IQR, interquartile range; Min, minimum; Max, maximum.
Regulatory T-Cell Profiles in SLE
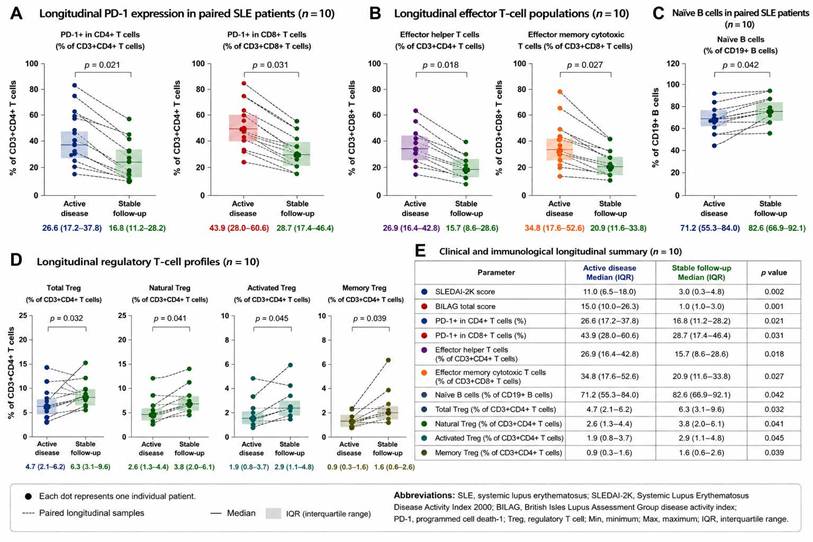
Substantial heterogeneity in Treg-associated immune profiles was observed across healthy controls and patients with SLE (Figure 4). Compared with healthy participants, several patients with SLE demonstrated relatively enriched activated and memory-associated Treg phenotypes during clinically active disease states. Paired longitudinal visualization further suggested dynamic variation in Treg-associated immune profiles between active disease and stable follow-up. In several patients, total Treg, natural Treg, activated Treg, and memory Treg populations demonstrated relative increases during stable follow-up in parallel with lower clinical disease activity. Nevertheless, considerable inter-individual variability remained evident, and heterogeneous longitudinal patterns were observed across individual patients.
Longitudinal immune profiling during active disease and stable follow-up in paired systemic lupus erythematosus samples. Paired longitudinal immune profiling was performed in patients with systemic lupus erythematosus (SLE, n = 10) using flow cytometry-based immunophenotyping. Individual paired blood samples obtained during clinically active disease and stable follow-up were analyzed descriptively to evaluate temporal immune variation within individuals. Each dot represents one individual patient, and dashed lines indicate paired longitudinal samples. Horizontal lines indicate the median, and shaded areas represent the interquartile range (IQR). P values were calculated using the Wilcoxon signed-rank test. (A) Longitudinal PD-1-associated immune markers, including PD-1⁺ CD4⁺ T cells and PD-1⁺ CD8⁺ T cells. (B) Longitudinal effector T-cell populations, including effector helper T cells and effector memory cytotoxic T cells. (C) Longitudinal naïve B-cell profiles. (D) Longitudinal regulatory T-cell (Treg)-associated immune profiles, including total Treg, natural Treg, activated Treg, and memory Treg populations. (E) Clinical and immunological longitudinal summary comparing clinically active disease and stable follow-up states, including SLEDAI-2K scores, BILAG total scores, and evaluated immune markers. Overall, clinically stable follow-up samples demonstrated reduced PD-1-associated and effector T-cell immune activation, accompanied by relative recovery of naïve B-cell and Treg-associated immune profiles. Abbreviations: SLE, systemic lupus erythematosus; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000; BILAG, British Isles Lupus Assessment Group disease activity index; PD-1, programmed cell death-1; Treg, regulatory T cell; IQR, interquartile range; Min, minimum; Max, maximum.
Integrated Analysis of PD-1 and Treg Profiles
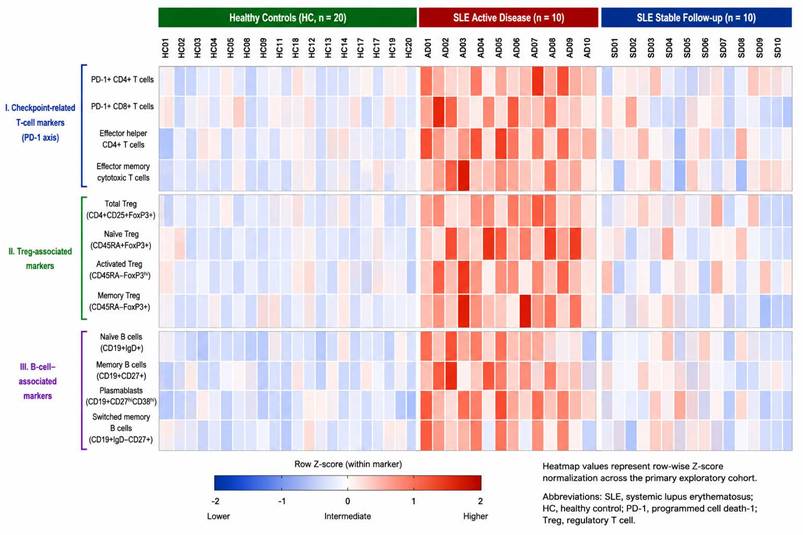
An integrated heatmap incorporating checkpoint-related T-cell markers, Treg-associated immune markers, and B-cell-associated immune populations was generated to visualize overall immune variation across healthy controls and patients with SLE (Figure 5). Healthy controls demonstrated relatively clustered immune distributions despite measurable inter-individual variability, whereas patients with SLE exhibited broader heterogeneity across checkpoint-related, regulatory, and B-cell-associated immune markers. In several patients with SLE, relatively higher positioning of PD-1-associated and Treg-associated immune markers, together with variation in selected B-cell-associated immune populations, was observed during clinically active disease states compared with stable follow-up. Longitudinal visualization further suggested partial normalization of selected immune profiles during stable follow-up, although substantial inter-individual variability remained evident and the magnitude of change varied across patients. Because heatmap visualization was based on row-wise normalized relative positioning rather than inferential statistical analysis, all observations are intended solely for descriptive pattern recognition and hypothesis generation.
Integrated heatmap visualization of immune marker distributions across healthy controls and systemic lupus erythematosus disease states. Integrated heatmap visualization of flow cytometry-based immune profiling across healthy controls (HC, n = 20), patients with active systemic lupus erythematosus (SLE active disease, n = 10), and paired clinically stable follow-up samples (SLE stable follow-up, n = 10). Samples were displayed according to predefined clinical grouping rather than unsupervised hierarchical clustering. Immune markers were functionally grouped into three major categories: (I) checkpoint-related T-cell markers (PD-1 axis), (II) regulatory T-cell (Treg)-associated markers, and (III) B-cell-associated markers. Heatmap values represent row-wise Z-score normalization within each immune marker across the primary exploratory cohort. Red coloration indicates relatively higher expression or abundance, whereas blue coloration indicates relatively lower expression relative to the cohort-wide distribution for each marker. Active SLE samples demonstrated increased PD-1-associated and effector immune activation patterns, while clinically stable follow-up samples showed partial normalization toward healthy control immune distributions. The heatmap illustrates inter-individual immune heterogeneity and longitudinal immune variation across disease activity states in this exploratory immunophenotyping cohort. Abbreviations: SLE, systemic lupus erythematosus; PD-1, programmed cell death-1; Treg, regulatory T cell.
Illustrative Immune Profiles in Selected Clinical Cases
In addition to the primary exploratory cohort, two representative clinical cases were descriptively retained to illustrate contextual immune variation under inflammatory and postoperative conditions. The infection-related case involved a 47-year-old male evaluated during recovery following surgical debridement for post-traumatic cellulitis. This case demonstrated relatively higher positioning of PD-1-associated immune markers across activated helper and cytotoxic T-cell populations compared with healthy reference distributions. Relatively increased activated Treg-associated and CD39⁺ regulatory immune populations were also observed during the recovery phase of localized inflammation (Table 2). In contrast, the postoperative case involved an 88-year-old female evaluated following vertebral compression fracture surgery and demonstrated broader heterogeneity across checkpoint-associated and regulatory immune markers. Compared with the infection-related case, relative positioning of PD-1-associated immune markers appeared less prominent, whereas mixed distributions of activated and memory-associated Treg populations remained evident (Table 2).
Clinical characteristics (A) and immunophenotypic profiles (B) of two representative clinical stress conditions.
| (A) Clinical Characteristics | |||
|---|---|---|---|
| Variable | Cellulitis (47-year-old male) | Elderly Postoperative (88-year-old female) | |
| Demographics | Previously healthy adult | Elderly individual with multiple comorbidities | |
| Primary condition | Post-traumatic cellulitis (right foot) | Osteoporotic vertebral fracture, postoperative state | |
| Clinical context | Acute infection with surgical intervention | Chronic inflammation, aging, recurrent infection | |
| Comorbidities | None documented | Paraplegia, pressure ulcers, UTI, osteoporosis, GERD, depression | |
| Type of stress | Acute inflammation + debridement | Chronic inflammation + surgery + aging | |
| Clinical course | Infection → CRP elevation → debridement → antibiotics → recovery | Surgery → immobilization → pressure ulcers → recurrent infection | |
| Treatment exposure | Debridement + antibiotics (ampicillin/sulbactam) | Multiple surgeries + antibiotics + long-term care | |
| CRP (mg/dL) | 4.5 | 7.8 | |
| WBC (×10³/μL) | 10.54 | 9.65 | |
| Infection status | Localized infection | Chronic/recurrent infection | |
| Timing of sampling | Post-infection recovery phase | Postoperative with ongoing inflammation | |
| (B) Immunophenotypic Profiles | |||
| Immune Parameter | Descriptive Interpretation | ||
| PD-1 expression | Increased relative to baseline | Higher relative levels observed | Consistent with checkpoint activation |
| Naïve T cells | Slightly lower relative levels | Lower relative levels observed | Compatible with age-related changes |
| Effector T cells | Higher relative levels | Lower relative levels | Distinct response patterns observed |
| Memory Tregs | Higher relative levels | Higher relative levels | Regulatory changes observed |
| Activated Tregs | Slightly higher relative levels | Higher relative levels | Sustained regulatory activity |
| Natural Tregs | Similar to or slightly higher | Higher relative levels | Compatible with aging-related remodeling |
| CD39⁺ Tregs | Higher relative levels | Higher relative levels | Suggestive of suppressive phenotype |
| Regulatory B cells | Slightly higher relative levels | Higher relative levels | Possible compensatory regulation |
| Plasmablasts | Similar to or slightly higher | Higher relative levels | Consistent with ongoing stimulation |
| Tr1 cells | Higher relative levels | Higher relative levels | IL-10-associated regulatory response |
Abbreviations: CRP, C-reactive protein; WBC, white blood cell count; UTI, urinary tract infection; GERD, gastroesophageal reflux disease; Tregs, regulatory T cells.
Reference ranges:
CRP, <0.5 mg/dL; WBC count, 4.0-10.0 × 10³/μL
All data are presented descriptively without formal statistical analysis due to the small sample size. Immunophenotypic findings represent relative differences compared with baseline observations and should be interpreted as exploratory and hypothesis-generating. Clinical variables were obtained from available medical records at the time of sampling.
An additional healthy participant of Ukrainian background was evaluated separately in supplementary analyses to provide a descriptive illustration of inter-individual immune variability. Compared with the healthy Taiwanese reference cohort, this participant demonstrated lower PD-1⁺ Effector Helper T-cell proportions and higher Memory Treg proportions (Supplementary Figure 1). Serial observations obtained during asymptomatic and mild upper respiratory symptom states further demonstrated temporal fluctuation in these immune markers. Because this supplementary observation was based on a single individual and included solely for descriptive visualization, the findings were not incorporated into formal statistical comparisons, inferential analyses, or cohort-level analyses.
Discussion
Baseline Variation in Immune Regulatory Profiles
Healthy controls demonstrated measurable inter-individual variability in PD-1 expression and Treg profiles despite the absence of overt inflammatory illness. Moderate variability was observed across effector T-cell populations and activated or memory Treg subsets, suggesting that baseline immune regulatory states may differ substantially between individuals. These findings are consistent with previous studies showing that immune system composition and responsiveness vary according to genetic background, environmental exposures, antigen experience, microbiome composition, and lifestyle-related factors [8-10,25,26]. Accordingly, variation in immune checkpoint signaling and Treg profiles may reflect host-specific immune regulatory characteristics rather than pathological immune dysregulation alone. Previous studies have also demonstrated that immune aging, immunosenescence, T-cell exhaustion, and population-level genetic adaptation can influence immune regulatory pathways and contribute to heterogeneity in immune phenotypes [35-41].
Because of the exploratory design and modest sample size, the determinants underlying immune heterogeneity could not be systematically evaluated. Therefore, these observations should be interpreted as descriptive rather than mechanistic or population-level findings.
Clinical Implications of Immune Regulatory Variation in SLE
Compared with healthy controls, patients with SLE demonstrated broader heterogeneity across checkpoint-related and regulatory immune markers, including variation in PD-1 expression and activated or memory Treg populations. Paired longitudinal observations further suggested that checkpoint-related and Treg profiles may vary dynamically across clinically active and stable disease states, although substantial inter-individual variability remained evident.
In several individuals, relative reductions in selected PD-1-related markers and activated Treg populations were observed during stable follow-up together with lower SLEDAI-2K and BILAG disease activity scores. However, persistent elevations and heterogeneous longitudinal patterns remained evident in some patients, highlighting the individualized and context-dependent nature of immune regulation in SLE.
These observations are broadly consistent with previous studies implicating T-cell dysregulation, regulatory T-cell imbalance, immune checkpoint pathways, and age-associated immune remodeling in autoimmune and immune-mediated diseases [21-23,38-41]. However, because of the exploratory design, modest cohort size, and absence of functional immune validation, the clinical implications of these findings remain preliminary and require confirmation in larger longitudinal cohorts.
Contextual Immune Variation in Illustrative Clinical Cases
Selected illustrative clinical cases involving post-infectious recovery and postoperative inflammatory conditions were included descriptively to provide contextual insight into immune heterogeneity under clinically relevant settings. Relative variation in PD-1-related markers and Treg profiles was observed compared with healthy reference distributions. The infection-related recovery case demonstrated relatively increased activated and memory Treg populations together with enriched PD-1-related markers across helper and cytotoxic T-cell subsets during recovery following localized cellulitis. In contrast, the postoperative case demonstrated broader heterogeneity across checkpoint-related and regulatory immune markers with mixed activated and memory Treg distributions.
An additional participant of Ukrainian background, evaluated separately in supplementary analyses, further illustrated measurable inter-individual immune variability under different physiological and mild inflammatory conditions. Relative variation in PD-1⁺ Effector Helper T-cell proportions and Memory Treg proportions was observed compared with the healthy Taiwanese reference cohort. Serial observations obtained during asymptomatic and mild upper respiratory symptom states further demonstrated temporal fluctuation in these immune markers. Because this supplementary observation was based on a single individual and was included solely for descriptive visualization, the findings should be interpreted cautiously as contextual observations rather than evidence of ethnicity-associated, population-level, or disease-specific immune differences.
Because these observations were derived from individual cases with heterogeneous clinical conditions and without standardized longitudinal validation, they should be interpreted cautiously as descriptive contextual findings rather than evidence of condition-specific or population-level immune responses.
Strengths and Limitations
This study has several strengths. First, the study adopted an exploratory longitudinal immunophenotyping framework to characterize PD-1 expression and Treg-associated immune profiles in patients with SLE relative to healthy controls, providing contextual insight into baseline immune variability. Second, the use of multiparameter flow cytometry enabled detailed characterization of PD-1 expression and multiple Treg-associated immune populations across representative immune regulatory compartments. Third, paired longitudinal immune profiling available in selected patients with SLE provided preliminary insight into temporal immune variation across clinically active and stable disease states. Fourth, individual-level visualization approaches—including paired longitudinal plots and integrated heatmaps—helped preserve inter-individual immune heterogeneity and facilitated descriptive interpretation within a modest exploratory cohort. Finally, the inclusion of illustrative inflammatory, postoperative, and supplementary contextual observations provided additional perspective on immune variability across distinct clinical settings and mild inflammatory conditions.
Several limitations should also be acknowledged. First, despite inclusion of a primary exploratory cohort, the overall sample size remained modest, limiting statistical power and generalizability. Second, the SLE cohort was clinically heterogeneous, and important confounding factors—including disease activity, medication exposure, comorbidities, inflammatory status, disease duration, and potential age and gender imbalance relative to healthy controls—may have influenced immune phenotypes and were not uniformly controlled. Third, although longitudinal follow-up data were available in selected patients, sampling intervals and treatment conditions were not fully standardized. Fourth, functional assays evaluating T-cell exhaustion, cytokine activity, suppressive immune function, or mechanistic signaling pathways were not performed; therefore, the observed immunophenotypic findings should not be interpreted as direct evidence of functional immune dysregulation. Fifth, statistical analyses were exploratory in nature, and no adjustment for multiple comparisons was performed because of the hypothesis-generating design and modest sample size of the study. Finally, the illustrative clinical cases and supplementary descriptive observations—including the additional participant of Ukrainian background—were based on individual-level observations and were included solely for contextual interpretation rather than inferential comparison.
Conclusion
This exploratory longitudinal immunophenotyping study describes inter-individual variation in PD-1 expression and Treg-associated immune profiles across healthy individuals and patients with SLE. Longitudinal observations further suggested dynamic immune variation between clinically active disease and stable follow-up states, highlighting the individualized and context-dependent nature of immune regulation in SLE.
Because of the exploratory design, modest cohort size, clinical heterogeneity, and absence of functional immune validation, these findings should be interpreted cautiously and considered hypothesis-generating rather than confirmatory. Nevertheless, the present study provides preliminary descriptive insight into immune regulatory variation in SLE and supports further investigation in larger, well-characterized longitudinal cohorts with standardized immune monitoring and functional immune assessment.
Abbreviations
HC: healthy controls; PD-1: programmed cell death-1; Treg: regulatory T cell; SD: standard deviation.
Supplementary Material
Supplementary figure and table.
Acknowledgements
Funding
This study was supported by the National Science and Technology Council, Taiwan (NSTC 112-2314-B-016-033, NSTC 113-2314-B-016-052, and NSTC 114-2314-B-016-052-MY3), Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan (TSGH-E-112218 and TSGH-E-113238), Ministry of National Defense, Medical Affairs Bureau (MND-MAB-E-115253), and the Research Fund of Taoyuan Armed Forces General Hospital (TYAFGH-D-115024 and TYAFGH-E-115051).
Author Contributions
Conceptualization, J.-W.L., Y.-J.H., P.-J.H., and F.-C.L.; data collection, S.-W.L., Y.-J.H., P.-J.H., and F.-C.L.; formal analysis, T.-Y.H. and W.-L.J.; methodology, A.B., Y.-J.H., and P.-J.H.; validation, J.-W.L., Y.-J.H., P.-J.H., and F.-C.L.; writing—original draft, J.-W.L., Y.-J.H., P.-J.H., and F.-C.L.; writing—review and editing, J.-W.L., S.-W.L., Y.-J.H., P.-J.H., and F.-C.L.; funding acquisition, P.-J.H. and F.-C.L. All authors have read and agreed to the published version of the manuscript.
Ethics Approval
The research protocol was reviewed and approved by the Ethics Committee of Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan (reference number: TSGHIRB-C202405129 and TSGHIRB-2-106-05-001). All procedures were conducted in accordance with the ethical standards of the institutional research committee and with the principles of the Declaration of Helsinki.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process
The authors used generative AI tools solely for language editing and improvement of manuscript clarity. The scientific content and conclusions were entirely generated and verified by the authors.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Ishida Y, Agata Y, Shibahara K, Honjo T. Induced expression of PD-1, a novel member of the immunoglobulin gene superfamily, upon programmed cell death. EMBO J. 1992;11:3887-95
2. Wherry EJ. T cell exhaustion. Nat Immunol. 2011;12:492-9
3. Ai L, Xu A, Xu J. Roles of PD-1/PD-L1 pathway: signaling, cancer, and beyond. Adv Exp Med Biol. 2024;1441:33-59
4. Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M. Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha-chains (CD25). J Immunol. 1995;155:1151-64
5. Brunkow ME, Jeffery EW, Hjerrild KA, Bennett DC, Clark LB, Ziegler SF. Disruption of a new forkhead/winged-helix protein, scurfin, results in the fatal lymphoproliferative disorder of the scurfy mouse. Nat Genet. 2001;27:68-73
6. Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and function of CD4⁺CD25⁺ regulatory T cells. Nat Immunol. 2003;4:330-6
7. Ramsdell F, Ziegler SF. FOXP3 and scurfy: how it all began. Nat Rev Immunol. 2014;14:343-9
8. Nédélec Y, Sanz J, Baharian G, Szpiech ZA, Pacis A, Dumaine A. et al. Genetic ancestry and natural selection drive population differences in immune responses to pathogens. Cell. 2016;167:657-69
9. Tsang JS, Schwartzberg PL, Kotliarov Y, Biancotto A, Chen J. et al. Global analyses of human immune variation reveal baseline predictors of postvaccination responses. Cell. 2014;157:499-513
10. Brodin P, Jojic V, Gao T, Bhattacharya S, Angel CJL. et al. Variation in the human immune system is largely driven by non-heritable influences. Cell. 2015;160:37-47
11. Hotchkiss RS, Monneret G, Payen D. Sepsis-induced immunosuppression: from cellular dysfunctions to immunotherapy. Nat Rev Immunol. 2013;13:862-74
12. Zhang H, Hu H, Jiang X, Wu Y, Xu C. et al. Sepsis-induced immunosuppression: mechanisms, diagnosis and current treatment options. Mil Med Res. 2022;9:56
13. Brahmamdam P, Inoue S, Unsinger J, Chang KC, McDunn JE, Hotchkiss RS. Delayed administration of anti-PD-1 antibody reverses immune dysfunction and improves survival during sepsis. J Leukoc Biol. 2010;88:233-40
14. Chen C, Chen D, Zhang Y, Liu Y, Zhao J. et al. Changes of CD4⁺CD25⁺FOXP3⁺ and CD8⁺CD28⁻ regulatory T cells in non-small cell lung cancer patients undergoing surgery. Int Immunopharmacol. 2014;18:255-61
15. Aw D, Silva AB, Palmer DB. Immunosenescence: emerging challenges for an ageing population. Immunology. 2007;120:435-46
16. Yousefzadeh MJ, Flores RR, Zhu Y, Schmiechen ZC, Brooks RW. et al. An aged immune system drives senescence and ageing of solid organs. Nature. 2021;594:100-5
17. Zhou W, Deng J, Chen Q, Li R, Xu X, Guan Y. et al. Expression of CD4⁺CD25⁺CD127low regulatory T cells and cytokines in peripheral blood of patients with primary liver carcinoma. Int J Med Sci. 2020;17:712-9
18. Chen Q, Mo L, Cai X, Wei L, Xie Z, Li H. et al. ICOS signal facilitates Foxp3 transcription to favor suppressive function of regulatory T cells. Int J Med Sci. 2018;15:666-73
19. Ding J, Dai J, Cai H, Gao Q, Wen Y. Extensively disturbance of regulatory T cells-Th17 cells balance in stage II pulmonary sarcoidosis. Int J Med Sci. 2017;14:1136-42
20. Liu CH, Weng JR, Wu LH, Song RY, Huang MD. et al. Arbutin overcomes tumor immune tolerance by inhibiting tumor programmed cell death-ligand 1 expression. Int J Med Sci. 2024;21:2992-3002
21. Sharabi A, Tsokos GC. T cell metabolism: new insights in systemic lupus erythematosus pathogenesis and therapy. Nat Rev Rheumatol. 2020;16:100-12
22. Miyara M, Gorochov G, Ehrenstein M, Musset L, Sakaguchi S, Amoura Z. Human FoxP3+ regulatory T cells in systemic autoimmune diseases. Autoimmun Rev. 2011;10:744-55
23. Suárez-Fueyo A, Bradley SJ, Tsokos GC. T cells in Systemic Lupus Erythematosus. Curr Opin Immunol. 2016;43:32-8
24. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R. et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheum Dis. 2019;78:1151-9
25. Tsang JS, Schwartzberg PL. Global immune variation and its implications for human disease. Trends Immunol. 2015;36:489-99
26. Brodin P, Davis MM. Human immune system variation. Nat Rev Immunol. 2017;17:21-9
27. Sakaguchi S, Wing K, Miyara M. Regulatory T cells: how do they suppress immune responses? Int Immunol. 2007;19:1025-34
28. Shevach EM. Mechanisms of Foxp3⁺ T regulatory cell-mediated suppression. Immunity. 2009;30:636-45
29. Josefowicz SZ, Lu LF, Rudensky AY. Regulatory T cells: mechanisms of differentiation and function. Annu Rev Immunol. 2012;30:531-64
30. Groux H, O'Garra A, Bigler M, Rouleau M, Antonenko S. et al. A CD4⁺ T-cell subset inhibits antigen-specific T-cell responses and prevents colitis. Nature. 1997;389:737-42
31. Miyara M, Yoshioka Y, Kitoh A, Shima T, Wing K, Niwa A. et al. Functional delineation and differentiation dynamics of human CD4+ T cells expressing the FoxP3 transcription factor. Immunity. 2009;30:899-911
32. Mauri C, Bosma A. Immune regulatory function of B cells. Annu Rev Immunol. 2012;30:221-41
33. Akbar AN, Henson SM. Are senescence and exhaustion intertwined or unrelated processes that compromise immunity? Nat Rev Immunol. 2011;11:289-95
34. McLane LM, Abdel-Hakeem MS, Wherry EJ. CD8 T cell exhaustion during chronic viral infection and cancer. Annu Rev Immunol. 2019;37:457-95
35. Blank CU, Haining WN, Held W, Hogan PG, Kallies A. et al. Defining T cell exhaustion. Nat Rev Immunol. 2019;19:665-74
36. Okada Y, Wu D, Trynka G, Raj T, Terao C. et al. Genetics of rheumatoid arthritis contributes to biology and drug discovery. Nature. 2014;506:376-81
37. Quach H, Rotival M, Pothlichet J, Loh YHE, Dannemann M. et al. Genetic adaptation and Neandertal admixture shaped the immune system of human populations. Cell. 2016;167:643-56
38. Baecher-Allan C, Hafler DA. Human regulatory T cells and their role in autoimmune disease. Immunity. 2006;24:471-80
39. Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378:158-68
40. Goronzy JJ, Weyand CM. Mechanisms underlying T cell ageing. Nat Rev Immunol. 2019;19:573-83
41. Fulop T, Larbi A, Dupuis G, Le Page A, Frost EH. et al. Immunosenescence and inflamm-aging as two sides of the same coin. Nat Rev Immunol. 2018;18:299-312
Author contact
![]() Corresponding author: Feng-Cheng Liu, MD, PhD, Rheumatology/Immunology and Allergy, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, No. 161, Section 6, Minquan East Road, Taipei 114, Taiwan, R.O.C. Tel: +886 287923100 ext. 12588, e-mail: lfc10399com.
Corresponding author: Feng-Cheng Liu, MD, PhD, Rheumatology/Immunology and Allergy, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical University, No. 161, Section 6, Minquan East Road, Taipei 114, Taiwan, R.O.C. Tel: +886 287923100 ext. 12588, e-mail: lfc10399com.