Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2010; 7(5):309-313. doi:10.7150/ijms.7.309 This issue Cite
Research Paper
Clinical Strategy for the Management of Solid Pseudopapillary Tumor of the Pancreas: Aggressive or Less?
Hong Chang1 ![]() , Yi Gong2, Jian Xu1, Zhongxue Su1, Chengkun Qin1, Zhenhai Zhang1
, Yi Gong2, Jian Xu1, Zhongxue Su1, Chengkun Qin1, Zhenhai Zhang1
1. Department of General Surgery, Shandong Provincial Hospital affiliated to Shandong University, Jinan Shandong, China;
2. Department of Rehabilitation, Shandong Provincial Hospital affiliated to Shandong University, Jinan Shandong, China.
Received 2010-5-14; Accepted 2010-8-27; Published 2010-9-1
Abstract
Objective: To further delineate the clinicopathological and radiological features of solid pseudopapillary tumor (SPT) of the pancreas and summarize the surgical therapy strategy for this tumor. Methods: A retrospective review of 18 pathologically confirmed cases of SPT was performed and the clinical and pathological features, radiological findings and surgical interventions were analyzed. Results: The patients included 17 females and 1 male with a median age of 23 years. The median diameter of the lesions was 8.0 cm. Abdominal pain was the predominant complaint (8/18). The rest of the patients were asymptomatic and presented with a pancreatic mass detected incidentally. Radiological study revealed a well-demarcated mass which was composed of a solid-cystic portion. On post-contrast CT, the solid portions could be enhanced whereas the cystic parts remained unenhanced. With the preoperative diagnosis of SPT in 11 patients and pancreatic cyst, benign or malignant pancreatic tumor in the rest, pancreatic tumor resection was successfully completed. Surgical exploration findings, pathological characteristics and good prognosis of the patients with SPT, indicated its low-grade malignant potential. Conclusion: In combination with clinical findings, radiological features of SPT may help to make the correct diagnosis and differentiation from other pancreatic neoplasms. Once diagnosed, given the excellent prognosis and low-grade malignancy, less aggressive surgical resection of the primary lesion is proposed.
Keywords: Diagnosis, Pancreas, Solid pseudopapillary tumor, Surgery
Introduction
Solid Pseudopapillary Tumor (SPT) of the pancreas is a very rare entity with a reported incidence of 0.13% to 2.7% of all pancreatic tumors,1 which was once described in many other terms, such as Frantz's tumor, solid and cystic tumor, papillary cystic neoplasm, and solid and papillary epithelial neoplasm.2 From 1996, the term of SPT was recommended by the WHO pancreatic working group and is being widely accepted in medical practice.3 Of note, in recent reports it has been concluded gradually that Solid Pseudopapillary Neoplasm of the pancreas (SPN) is the correct description regarding the terminology.4,5,6 Despite the increases in recognition of characteristics of this tumor, which include a distinct female preponderance and low malignant potential, there is an increasing incidence of the disease reported 7 and the rate of preoperative misdiagnosis is rather high.2,8 Some clinicians have little knowledge about SPT,2,9 which might in turn result in the uncertainty of the strategy for its treatment. While further delineating the clinicopathological and radiological features, and summarizing the surgical therapy strategy of this tumor, we hereby report our experience in the treatment of 18 cases of SPT retrospectively along with review of the literatures.
Methods
A retrospective review of 18 pathologically confirmed cases of SPT treated at the Department of General Surgery, Shandong Provincial Hospital, Shandong University, from January 1, 2000 to January 20, 2010, was performed. The clinicopathological features, radiological findings and surgical interventions were analyzed. All of the patients were closely followed up at regular intervals. The review was based on clinic records or telephone interviews. The post operative follow up periods ranged from 4 months to 9 years.
Results
The patients included 17 females and 1 male, with a median age of 23 years (range 13-59). All patients underwent testing for blood sugar, serum and urine amylase, tumor markers (AFP, CEA, CA199, CA125) and the level of detections were all within normal limits. The median diameter of the lesions was 8.0 cm (range 4-20). Nine patients had their tumors within the head, 2 in the body and 7 in the tail of the pancreas. Notably one patient was demonstrated to have liver metastasis. The predominant presenting complaint was abdominal pain (8/18). The rest of the patients were asymptomatic and tumors were detected incidentally during routine physical examination. All these patients had no other obvious symptoms including weight loss, diarrhea, or general weakness. Obstructive jaundice was not observed in any of these cases, notably one patient with the tumor located in the pancreatic head had a dilated Common Bile Duct (CBD) and Pancreatic Duct (PD) (1.5 and 0.3 cm in diameter respectively).
Among the 18 cases of SPT, abdominal ultrasonography and CT scan were both performed in 16 of the 18 patients. In the rest of two patients, ultrasonography was carried out and revealed a solid-cystic neoplasm of the pancreas. 3 patients in all 18 cases underwent ultrasonography, CT and MRI for differentiation diagnosis. Radiological studies revealed a well-demarcated mass, which was composed of a solid-cystic portion. 11 patients were correctly diagnosed with a SPT by CT scan. MRI indicated the diagnosis of SPT in three patients. Notably, it was CT scan that delineated the liver metastasis, whereas ultrasound gave a negative result. With the preoperative diagnosis of SPT in 11 patients and pancreatic cyst, benign or malignant pancreatic tumor in the rest, tumor resection was completed successfully. Four patients underwent a distal pancreatectomy combined with splenectomy, 3 patients underwent a spleen-preserving distal pancreatectomy, 9 patients underwent a local tumor excision. The patient presenting with liver metastasis underwent resection of both the primary lesion and the liver metastasis. One patient underwent a duodenum-preserving resection of pancreatic head.
On surgical exploration, no severe adhesion or invasion of the SPT to the adjacent organs and near-by vessels was grossly noted, the exception being one distant metastasis to the left robe of liver was found. Lymph node enlargements were confirmed to be benign, reactive hyperplasia on pathology. Post operative complications included 4 pancreatic fistulas which were managed conservatively and resolved within 1 month, 2 months, 4 months and 6 months, respectively. The remaining 14 patients were discharged without remarkable complications within two weeks of their operation.
Grossly, SPT appeared encapsulated beneath a smooth glistening surface and had well-defined margins. Microscopically the tumor was composed of nests of epithelial cells with a solid pseudopapillary cystic and trabecular pattern, which demonstrated the characteristics of SPT histologically.
At a median follow-up period of 3.4 years (range 0.3-9 years) for all 18 patients, no mortality or local recurrence or distant metastasis were found.
Discussion
After SPT was finally added to the definitions under the current classification of pancreatic neoplasm from WHO (1996), the increasing awareness of the clinical and pathological features of this rare neoplasm might help to differentiate it from other pancreatic tumors. The most common symptoms of SPT, reportedly, but less peculiar, included abdominal pain, or a palpable abdominal mass.7,10,11 However, approximately 20% of patients were free from symptoms but were only incidentally detected by laparotomy or radiographic examination.11 SPT usually predominates in adolescent girls and young women and less common in males.8,10,11,12.13 However, in one retrospective review, the patients with SPT presented with a median age of 39 years, which is significantly older than in the other reported series.7 Literatures showed the head and tail of the pancreas were the preferential sites of the occurrence of SPT.3,7,10,14,15,16 In our series, the presenting clinical and pathological characteristics of SPT were consistent with those most mentioned above. In general, our hereby reported experience suggests, when a young female patient presents with a mixed solid and cystic pancreatic mass, whether she is asymptomatic or with abdominal pain, which might be located in any portion of the pancreas, especially in the head or tail, the diagnosis of SPT should be suspected and confirmed by further investigations. In our series, there was only 1 male confirmed to have SPT.
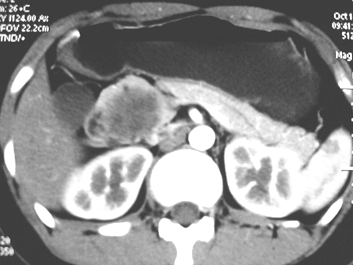
In combination with clinical findings, radiological features of SPT may help to make the correct diagnosis and differentiation from other pancreatic neoplasms. Abdominal ultrasound and CT scan usually demonstrate a huge, well-encapsulated mass with both solid and cystic components and displacement of nearby structures.15,17 Additionally, CT can play much more important role by providing further information about the size, location, the local invasion and vessel involvement of SPT, ultimately help to provide the final treatment strategy. In this study, on pre-contrasted CT, solid and cystic structures were demonstrated in 7 patients with SPT. After enhancement, solid and cystic structures were shown in 11 patients. Especially, the solid portions were moderately or obviously enhanced whereas the cystic parts remained unenhanced (Fig.1), which were consistent with those reported previously.9,11,18 It was mentioned accompanying CBD dilation and intra tumor calcification were infrequent findings in SPT patients.9,11,15,19 In our study, only one SPT patient with a tumor located in the pancreatic head presented with dilation of CBD. Of note, internal or capsular calcification was shown in 5 patients (Fig.2), suggesting the role of calcification on the development of SPT might need to be further investigated. Considering the superiority of MRI in terms of correlation between radiological and clinicopathological findings in SPT, MRI was strongly proposed for the diagnosis of SPT.6,10,18 Consistently, in our study, the diagnosis of SPT suggested by MRI was ultimately confirmed pathologically.
The CT scan demonstrated the solid portion of SPT was moderately or obviously enhanced whereas the cystic part remained unenhanced
The CT scan indicated the typical internal or capsular calcification in the SPT.

Once the diagnosis of SPT is made, surgery is the first choice of treatment, since other adjuvant therapies, including chemotherapy and radiotherapy, had shown no demonstrable response.7 According to the location of the tumor, distal pancreatectomy with splenectomy, pylorous preserving pancreatoduodenectomy, Whipple's operation or enucleation can be performed consquently.15 Furthermore, many reports had demonstrated less aggressive surgical procedures could be preferred for the treatment of SPT. 12,20 Considering the low-grade malignancy and good prognosis of SPT, moreover, the mass is usually well-demarcated from the surrounding pancreatic parenchyma, we performed less aggressive surgical resection to remove SPT. However, after the removal of pancreatic lesion, frozen section was routinely performed to rule out pancreatic malignancy. Otherwise, for the patients with pancreatic malignancies, a radical surgery should be the reasonable option for curative therapy. Aside from the distal pancreatectomy combined with splenectomy, for instance, regarding the reduction of risk of post-splenectomy sepsis and hematological disorders,21,22 and based on whether the vessels of the spleen could be divided and preserved, spleen-preserving distal pancreatectomy was attempted for three SPT patients in whom the mass was located in the portion of body or tail of the pancreas. For tumors of SPT located in the neck and body of the pancreas, resection of the midportion of the pancreas and the mass with preserving the rim of the head and tail portion can be achieved. However, for the patient in whom the mass was located within the head of the pancreas, given the low malignancy, well-defined margin and no invasion to adjacent structures, especially no indications of dilated CBD and PD indicating that the lesion had no close relation with the ducts, local tumor enucleation other than aggressive pancreatoduodenectory or Whipple's procedure was completed successfully without damaging of CBD and PD in 8 patients. For the patient in whom the CBD and PD were dilated, local enucleation was firstly completed with the preservation of the intact CBD, whereas the pancreatic duct was unfortunately found damaged. Subsequently, duodenum-preserving pancreatic head resection was performed and the postoperative recovery was uneventful.
Of note, up to 15% of cases of SPT have shown aggressive behavior consisting of extension into adjacent blood vessels and organs, local recurrence and distant metastasis.3,7,23,24 In our series, only one patient with the primary lesion in pancreatic head and liver metastasis was noted preoperatively. Consequently, enucleation of the local resection of SPT and liver metastasis was completed. An excellent outcome has been achieved with 11 months follow-up at the time writing this review. Given the reports that even patients with SPT with local recurrence as well as liver and peritoneal metastasis could still have long-term survival,25 the presence of metastasis in the SPT patients is not a contraindication for surgery. In these cases with metastasis, complete resection of both primary tumor and metastasis lesions, if possible, is proposed. Long-term survival might be achieved with an aggressive approach to both the primary lesion and to the synchronous or metachronous metastatic lesion, predominantly found in liver.7 However, as liver metastasis is quite uncommon with SPT (SPN), the experience with the management of disseminated disease is very limited in the literature6, therefore, attention to the therapy strategy of this neoplasm in the future may allow a more reasonable statement to be made.
In conclusion, SPT of the pancreas has atypical clinical symptoms, however, the characteristic imaging features can help to make the correct diagnosis of SPT and differentiate from other pancreatic tumors. Once diagnosed, given the excellent prognosis and low-grade malignancy, less aggressive surgical resection of the primary lesion is proposed. Whereas, for the SPT patients with distant metastasis or adjacent organ invasion, aggressive approach should be considered for long-term survival.
Acknowledgements
We thank Debbie Steele, Shannon Steele and Allyson & Eric Luedtke for editing this manuscript.
Conflict of Interest
The authors have declared that no conflict of interest exists.
References
1. Crawford BE2nd. Solid and papillary epithelial neoplasm of the pancreas, diagnosis by cytology. South Med J. 1998;91:973-937
2. Cheng DF, Peng CH, Zhou GW. et al. Clinical misdiagnosis of solid pseudopapillary tumour of pancreas. Chin Med J. 2005;118:922-926
3. Salla C, Chatzipantelis P, Konstantinou P. et al. Endoscopic ultrasound-guided fine-needle aspiration cytology diagnosis of solid pseudopapillary tumor of the pancreas. A case report and literature review. World J Gastroenterol. 2007;13:5158-5163
4. Sarr MG, Warshaw AL. Tumor versus neoplasm: isn't it time to use the correct term-neoplasm? Surgery. 2005;137:297
5. Tipton SG, Smyrk TC, Sarr MG. et al. Malignant potential of solid pseudopappillary neoplasm of the pancreas. Br J Surg. 2006;93:733-37
6. de Castro SMM, Singhal D, Aronson DC. et al. Management of Solid-pseudopapillary Neoplasms of the pancreas: a comparison with standard pancreatic neoplasms. World J Surg. 2007;31:1129-1134
7. Martin RC, Klimstra DS, Brennan MF, Conlon KC. Solid-pseudopapillary tumor of the pancreas: A surgical enigma? Ann Surg Oncol. 2002;9:35-40
8. Yang F, Fu DL, Jin C. et al. Clinical experiences of solid pseudopapillary tumors of the pancreas in China. J Gastroenterol Hepatol. 2008;23:1847-1851
9. Chen SQ, Zou SQ, Dai QB, Li H. Clinical analysis of solid-pseudopapillary tumor of the pancreas: report of 15 cases. Hepatobilliary Pancreat Dis Int. 2008;7(2):196-200
10. Yu CC, Yeh CN, Hwang TL, Jan YY. Clinicopathological study of solid and pseudopapillary tumor of pancreas: Emphasis on magnetic resonance imaging findings. World J Gastroenterol. 2007;13:1811-1815
11. Dong DJ, Zhang SZ. Solid-pseudopapillary tumor of the pancreas:CT and MRI features of 3 cases. Hepatobilliary Pancreat Dis Int. 2006;5:300-304
12. Zhang H, Liang TB, Wang WL. et al. Diagnosis and treatment of solid-pseudopapillary tumor of the pancreas. Hepatobilliary Pancreat Dis Int. 2006;5:454-458
13. Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of the pancreas: review of 718 patients reported in English literature. J Am Coll Surg. 2005;200:965-972
14. Kosmahl M, Pauser U, Peters K. et al. Cystic neoplasms of the pancreas and tumor-like lesion with cystic features: A review of 418 cases and a classification proposal. Virchows Arch. 2004;445:168-178
15. Lee W, Park Y, Choi J, Chi H, Kim B. Solid and papillary neoplasms of the pancreas. Yonsei Medical J. 1996;37:131-141
16. Lee SE, Jang JY, Huang DW, Park KW, Kim SW. Clinical features and outcome of solid pseudopapillary neoplasm: differences between adults and children. Arch Surg. 2008;143:1218-1221
17. Huang HL, Shih SC, Chang WH, Wang TE, Chen MJ, Chan YJ. Solid-pseudopapillary tumor of the pancreas: Clinical experience and literature review. World J Gastroenterol. 2005;11:1403-1409
18. Buetow PC, Buck JL, Pantongrag-Browa L, Beck KG, Ros PR, Adair CF. Solid and papillary epitheliar neoplasm of the pancreas: imaging-pathologic correlation on 56 cases. Radiology. 1996;3:707-711
19. Coleman KM, Poherty MC, Bigler SA. Solid-pseudopapillary tumor of the pancreas. Radiographics. 2003;23:1644-1648
20. Lee SE, Jang JY, Lee KU, Kim SW. Clinical comparison of distal pancreatectomy with or without splenectomy. J Korean Med Sci. 2008;23:1011-1014
21. Kimura W, Inoue T, Futakawa N, Shinkai H, Han I, Muto T. Spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein. Surgery. 1996;120:885-890
22. Warshaw AC. Conservation of the spleen with distal pancreatectomy. Arch Surg. 1998;123:550-553
23. Lam KY, Lo CY, Fan ST. Pancreatic solid-cystic-papillary tumor: clinicopathologic features in eight patients from Hong Kong and review of the literature. World J Surg. 1999;23:1045-1050
24. Pasquiou C, Scazec JY, Gentil-Perret A. et al. Solid pseudopapillary tumors of the pancreas. Pathology reports of 13 cases. Gastroenterol Clin Biol. 1999;23:207-214
25. Gonzalez-Campora R, Rios Martin JJ, Villar Rodriguez JL. et al. Papillary cystic neoplasm of the pancreas with liver metastasis coexisting with thyroid papillary carcinoma. Arch Pathol Lab Med. 1995;119:268-273
26. Machado MC, Machado MA, Bacchella T. et al. Solid pseudopalliary neoplasm of the pancreas: distinct patterns of onset, diagnosis, and prognosis for male versus female patients. Sugery. 2008;143:29-34
Author contact
![]() Corresponding author: Hong Chang, Department of General Surgery, Shandong Provincial Hospital, Shandong University. 324, Jing5Wei7 Road, Jinan Shandong, China. Tel: 531-85186363. Email: changhongedu.cn
Corresponding author: Hong Chang, Department of General Surgery, Shandong Provincial Hospital, Shandong University. 324, Jing5Wei7 Road, Jinan Shandong, China. Tel: 531-85186363. Email: changhongedu.cn